
Table of Contents
-
The part nobody prepares us for
-
Perimenopause vs menopause: what is the difference?
-
Why does this happen: the hormone changes behind the symptoms
-
Symptoms you might notice during the transition
-
What can help: evidence-based treatment options
-
Medical interventions
-
Lifestyle and holistic support
-
When to see a doctor
-
Expert FAQ
-
Final thoughts
The part nobody prepares us for
Menopause is often talked about as if it is one single moment. One day you are “fine,” and the next day you have crossed some invisible line into a new stage of life. But for most of us, that is not how it unfolds at all.
What many women actually live through is a long, confusing transition that can stretch over several years. Periods change. Sleep changes. Mood changes. Your body can start to feel unfamiliar before you have missed enough periods even to be called “in menopause.” That experience is real, common, and deeply under-explained. (nhs.uk)
In this guide, we will walk through the difference between perimenopause and menopause, why symptoms can begin years earlier than expected, what is happening hormonally, what treatments are backed by evidence, and when symptoms should not be brushed off. The goal is simple: to help us understand what our bodies are doing, so we can respond with clarity instead of confusion. (nhs.uk)
Perimenopause vs menopause: what is the difference?
a. Perimenopause
Perimenopause is the transition leading up to menopause. During this phase, the ovaries gradually become less consistent in releasing eggs and producing hormones, especially oestrogen and progesterone. It often begins in the 40s, but timing varies. ACOG notes that perimenopause may last from about ages 45 to 55, although some women notice changes earlier. (ACOG)
This is why many women say, “I do not feel like myself anymore,” even while they are still having periods. You can absolutely be in perimenopause while still menstruating. In fact, irregular or changing periods are often one of the earliest signs. (nhs.uk)
b. Menopause
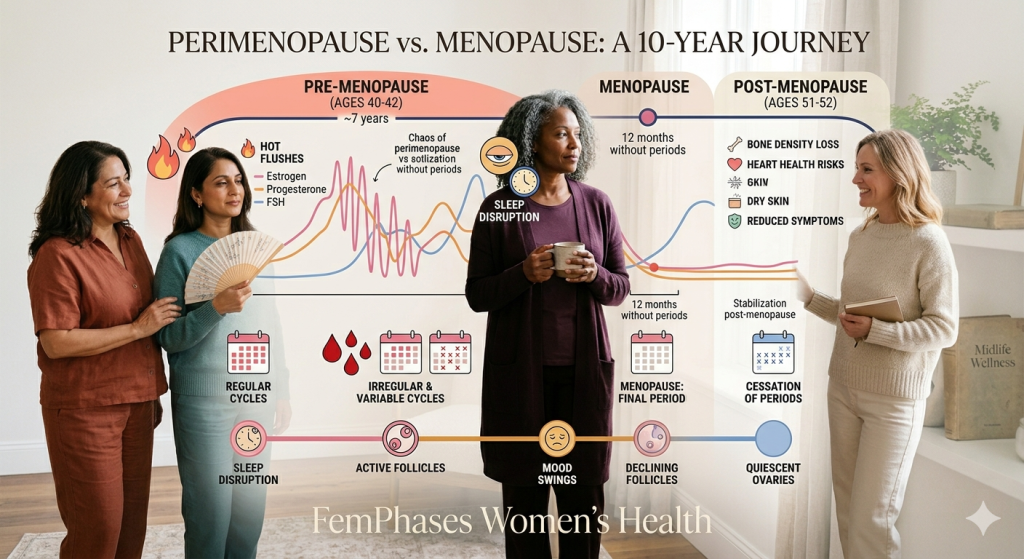
Menopause is not the whole transition. It has a specific medical definition: the point when you have gone 12 months in a row without a menstrual period. After that point, you are considered postmenopausal. (nhs.uk)
That distinction matters. Perimenopause is the lead-up. Menopause is the milestone. Post menopause is what comes after.
Perimenopause Symptom Checker
Why it feels like a “10-year transition”
People often describe this as a decade-long shift because symptoms may begin years before the final period and persist afterwards. NHS and NIH guidance both note that symptoms can start years before periods stop and may carry on beyond that point. (nhs.uk)
Whydoes this happen: the hormone changes behind the symptoms
This is the part we deserve to have explained clearly.
During the reproductive years, oestrogen and progesterone rise and fall in a more predictable rhythm. In perimenopause, that rhythm becomes less steady. The ovaries start working less reliably, ovulation becomes more irregular, and hormone levels fluctuate more dramatically. That hormonal unpredictability is what drives so many of the symptoms. (ACOG)
Oestrogen affects much more than periods. It interacts with the brain, blood vessels, bones, bladder, vagina, skin, sleep regulation, and temperature control. So when oestrogen swings up and down, it can show up as hot flushes, night sweats, anxiety, low mood, sleep disruption, vaginal dryness, joint discomfort, and brain fog. (nhs.uk)
Progesterone also changes. Because ovulation becomes less predictable, progesterone can drop unevenly as well. That can contribute to cycle changes, sleep disruption, and a general sense that your body is no longer running on the patterns you knew for years.
This is also why one blood test often does not “capture” what is happening. NICE advises that in people aged 45 or over with typical symptoms, menopause and perimenopause are usually diagnosed based on symptoms and menstrual history rather than broad hormone testing. (NICE)
Symptoms you might notice during the transition
The symptoms of menopause and perimenopause can be physical, emotional, cognitive, and sexual. They also vary widely. Some women have a few mild symptoms. Others feel as though every system in their body has changed at once. NHS, ACOG, and NIH sources describe a broad symptom pattern that can include: (nhs.uk)
- Irregular periods
- Heavier or lighter bleeding than usual
- Hot flushes
- Night sweats
- Sleep problems or waking at 3 a.m. for no obvious reason
- Mood changes, including irritability, anxiety, or low mood
- Brain fog, poor concentration, or forgetfulness
- Reduced libido
- Vaginal dryness
- Pain during sex
- Urinary symptoms, including urgency or recurrent discomfort
- Palpitations
- Headaches
- Aches, stiffness, or joint discomfort
- Changes in body composition or weight distribution
- Low confidence or a sense of not feeling like yourself
None of this means you are failing to cope. It means the transition is affecting real biology.
What can help: evidence-based treatment options
There is no single “right” way to move through menopause. Treatment should be based on symptoms, medical history, personal preference, and what matters most in your daily life. NICE recommends individualised menopause care and shared decision-making rather than a one-size-fits-all approach. (NICE)
A. Medical interventions
i. Hormone replacement therapy (HRT)
For many women, HRT is the most effective treatment for vasomotor symptoms such as hot flushes and night sweats. NICE recommends offering HRT for menopause-related vasomotor symptoms, and ACOG describes hormone therapy as a standard treatment option for several common symptoms. (NICE)
HRT may also help with:
- Sleep disrupted by hot flushes
- Vaginal dryness and discomfort
- Mood symptoms linked to the transition
- Bone protection in some women, especially when menopause happens early (ACOG)
There are different forms:
- Oestrogen-only HRT is usually used if you no longer have a uterus.
- Combined oestrogen and progestogen HRT is used if you still have a uterus, because oestrogen alone can thicken the uterine lining and raise endometrial cancer risk (ACOG)
Transdermal options, such as patches or gels, may be preferred in some people because the route of administration can affect clotting risk. ACOG notes that oral oestrogen may have a more prothrombotic effect than transdermal oestrogen. (ACOG)
ii. Vaginal oestrogen
If your main symptoms are vaginal dryness, burning, urinary irritation, or pain with sex, local vaginal oestrogen can be very effective and uses much lower systemic exposure than whole-body HRT. (National Institute on Ageing)
B. Nonhormonal prescription options
If HRT is not suitable, not wanted, or not the best fit, there are still evidence-based options. NHS and NIH note that some nonhormonal medicines may help with hot flushes and related symptoms, depending on individual circumstances. (nhs.uk)
C. CBT and symptom-focused support
NICE now recommends considering menopause-specific cognitive behavioural therapy (CBT) for vasomotor symptoms and recognises its role for sleep and depressive symptoms associated with menopause. CBT does not “fix” hormones, but it can reduce the distress and disruption symptoms cause. (NICE)
D. Surgery
Surgery is not a treatment for natural menopause symptoms. But if someone has surgery that removes both ovaries, menopause can happen suddenly because ovarian hormone production drops abruptly. That is a very different experience from the more gradual perimenopausal transition and should be discussed individually with a clinician. (National Institute on Ageing)
Why Am I Sweating at Night? Causes, Menopause and What Helps
Lifestyle and holistic support
Lifestyle support is not a substitute for medical care when symptoms are severe. But it can make a meaningful difference and support long-term health during and after menopause. Both the NHS and NIH recommend a healthy diet, physical activity, and attention to bone and heart health during this stage. (nhs.uk)
i. Nutrition
Aim for a pattern of eating that supports energy, blood sugar stability, bone health, and cardiovascular health. That generally means:
- regular meals
- enough protein
- calcium-rich foods
- vitamin D as appropriate
- fibre-rich plant foods
- limiting excess alcohol if it worsens sleep or hot flushes (National Institute on Ageing)
ii. Exercise
Movement helps more than weight alone. It supports sleep, mood, bone strength, heart health, and physical function. Weight-bearing and resistance exercise are especially valuable during and after menopause. (National Institute on Ageing)
iii. Sleep and stress regulation
Night sweats, anxiety, and early waking can feed each other. Gentle sleep routines, a cool bedroom, reducing alcohol late in the evening, and structured support for stress can all help. NIH specifically notes that hot flashes and mood changes can contribute to poor sleep. (National Institute on Ageing)
iv. Supplements: a balanced view
Many women look to supplements because they want something “natural.” That wish makes sense. But natural does not always mean effective, well-studied, or safe. It is worth checking evidence, interactions, and quality before trying supplements, especially if you have a history of breast cancer, blood clots, liver disease, or take regular medication.
Also, be cautious with compounded bioidentical hormones marketed as safer or more natural. ACOG advises against routine use of compounded bioidentical menopausal hormone therapy when approved therapies are available, because of concerns around regulation, dosing consistency, and evidence quality. (ACOG)
When to see a doctor
Please do not assume every midlife symptom is “just menopause.”
See a clinician if:
- your symptoms are affecting your work, sleep, relationships, or daily functioning
- you think you may be in perimenopause or menopause and want support
- you want to discuss whether HRT is appropriate for you
- symptoms begin before age 45, or especially before age 40, because early menopause or primary ovarian insufficiency may need assessment and treatment (NICE CKS)
Hormone Replacement Therapy (HRT) and contraception: Do you need birth control in perimenopause?
Red-flag symptoms that should not be ignored
Seek medical advice promptly if you have:
- bleeding after menopause, even once
- very heavy bleeding, bleeding between periods, or bleeding that feels unusual for you
- pelvic pain, pressure, or bloating that persists
- new breast changes
- chest pain, shortness of breath, or one-sided leg swelling
- severe low mood, depression, or thoughts of self-harm (nhs.uk)
Postmenopausal bleeding deserves special emphasis. NHS states that any vaginal bleeding after menopause should be checked by a doctor, even if it happens only once or is just light spotting, because although it is often not serious, it can be a sign of cancer. (nhs.uk)

Frequency Asked Questions
Is perimenopause the same as menopause?
No. Perimenopause is the transition leading up to menopause. Menopause is reached after 12 straight months without a period. (nhs.uk)
Can you still get pregnant during perimenopause?
Yes. If you are still ovulating, pregnancy is still possible. Changes in cycle length do not necessarily indicate that fertility is zero until menopause has been reached. (ACOG)
How long does perimenopause last?
It varies. ACOG notes that perimenopause may last from about ages 45 to 55, but timing differs from person to person. Symptoms may begin years before the final period. (ACOG)
Do I need a hormone blood test to know if it is menopause?
Usually not if you are 45 or older and have typical symptoms or period changes. NICE advises against using many routine hormone tests to identify perimenopause or menopause in this group. (NICE)
What is the most effective treatment for hot flushes?
For many women, HRT is the most effective treatment for hot flushes and night sweats. But the best treatment depends on your symptoms, risk factors, and preferences. (NICE)
Final thoughts
The transition into menopause is not all in your head, and it is not something you are supposed to endure in silence. For many of us, it begins long before the final period and touches sleep, mood, memory, sex, confidence, and daily comfort in ways that can feel surprisingly intense.
The good news is that support exists. There are evidence-based treatments, practical lifestyle tools, and compassionate ways to make sense of what is happening. Understanding the difference between perimenopause and menopause is often the first real moment of relief, because once we can name the transition, we can finally start responding to it with the care it deserves.
Disclaimer: This content is for informational purposes only and does not constitute medical advice.






