Introduction
If you have been feeling unlike yourself lately, you are not imagining it. Many of us notice changes in our cycles, mood, sleep, breasts, skin, or energy and wonder whether our Hormone Health is shifting underneath it all. When people use the phrase “oestrogen dominance,” they are usually describing a pattern where oestrogen’s effects feel stronger because progesterone is too low, especially in the second half of the cycle or during perimenopause. Strictly speaking, oestrogen dominance is not a formal medical diagnosis, but the symptoms people mean by it can be very real and deserve proper assessment. (The Menopause Consortium)
In this guide, we will walk through 12 common signs that progesterone may be too low, explain the biology in clear language, and cover both evidence-based medical options and supportive lifestyle steps to help you feel steadier, more informed, and in control of your Hormone Health. We will also cover the important red flags that should not be brushed aside.
Oestrogen Balance Self Assessment
Why this happens: the hormone mechanism in plain English
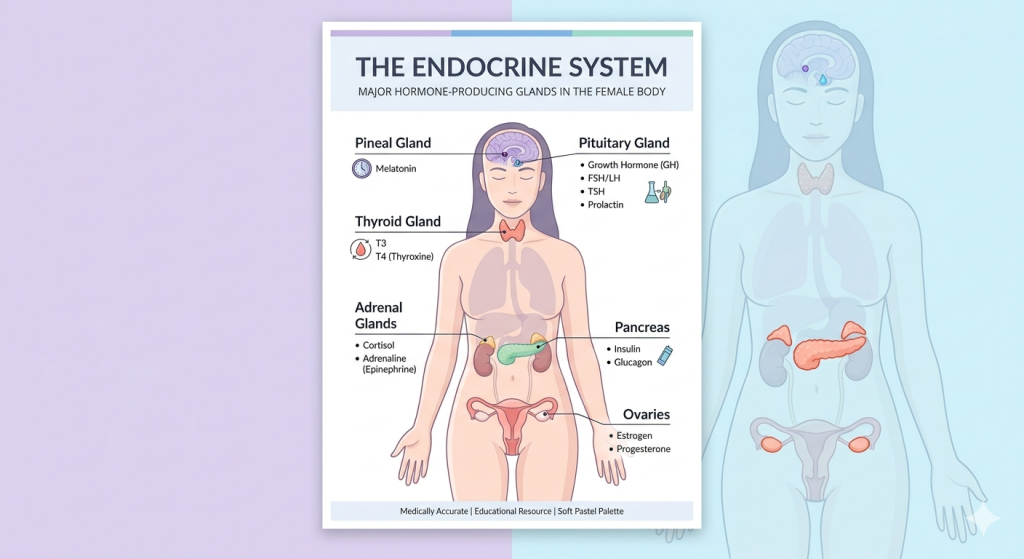
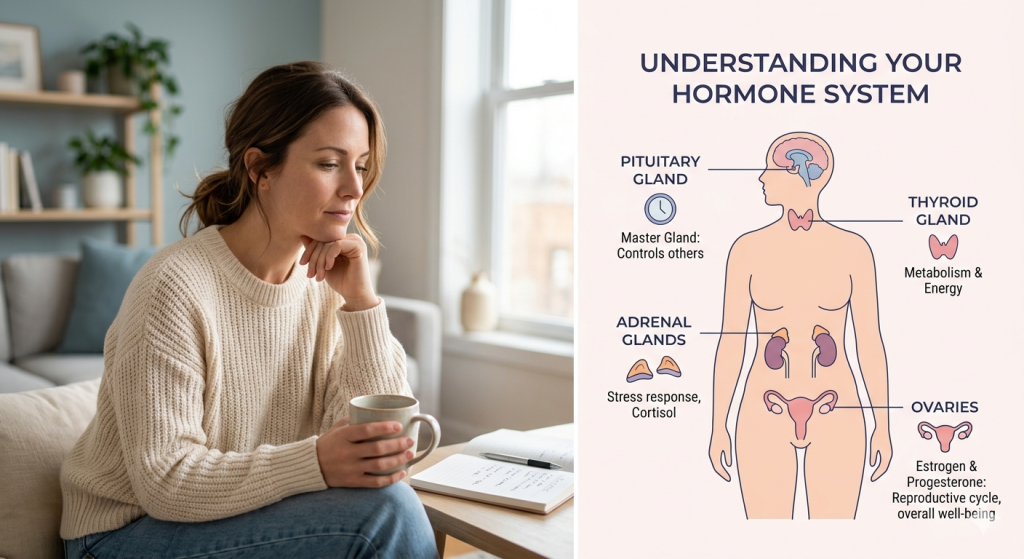
Oestrogen and progesterone are not “good” and “bad” hormones. They are a team. Oestrogen helps build up the uterine lining and plays a role in bone health, brain function, skin, and metabolism. Progesterone rises after ovulation and helps balance that build-up, stabilise the lining, and prepare the body for a possible pregnancy. (Cleveland Clinic)
When you do not ovulate regularly, you may not make enough progesterone. That can happen in perimenopause, with some cases of PCOS, during times of major stress, after significant weight change, with thyroid issues, or when cycles become irregular for other reasons. The result is not always “too much oestrogen” in an absolute sense. Often, there is too little progesterone relative to oestrogen’s effects. (Endocrine)
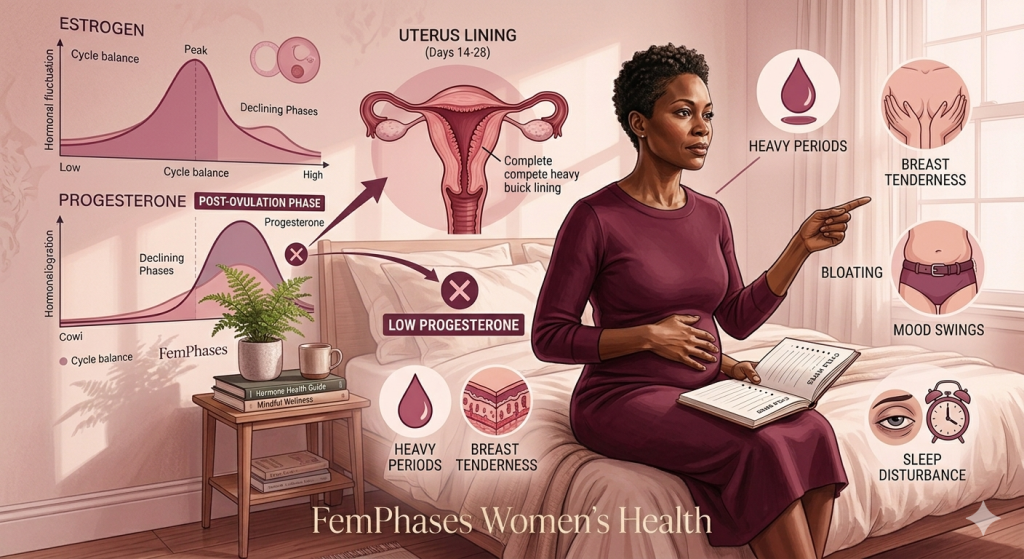
This matters because progesterone helps keep the uterine lining from being overstimulated. Without enough progesterone, some people develop heavier periods, more spotting, breast tenderness, bloating, and cycle-related mood changes. In menopause care, this is also why people with a uterus who take systemic oestrogen usually need a progestogen alongside it to protect the endometrium. (NICE)
So if your Hormone Health feels off, the issue may not be a trendy hormone label. It may be a very understandable pattern of ovulation changes, low progesterone, changing cycle signals, or a separate gynaecological condition that needs treatment.

12 signs your progesterone may be too low
Below are the symptoms many women describe when they talk about “oestrogen dominance.” None of these signs proves a diagnosis on its own, but together they can paint a useful picture.
- Heavy periods
- If you are soaking through pads or tampons faster than usual, passing clots, or finding your periods are disrupting work, sleep, or daily life, low progesterone can be part of the story because the uterine lining may be less well-regulated. Heavy bleeding is not considered normal and deserves assessment. (acog.org)
- Shorter cycles or more frequent periods
- Some women notice their cycle shortening, for example, from 28 days to 24 or 21 days. This can happen when ovulation becomes less predictable and progesterone support in the second half of the cycle drops. (acog.org)
- Spotting before your period
- Brown spotting or light bleeding in the days leading up to a period can sometimes indicate a weaker luteal phase, meaning progesterone may not stay high enough for long enough. (Endocrine)
- Breast tenderness or swollen breasts
- Sore, full, or lumpy-feeling breasts often get worse when hormonal balance is shifting. Breast tenderness is commonly reported with hormone fluctuations and can be especially noticeable in perimenopause. (nhs.uk)
- Bloating and fluid retention
- Feeling puffy, swollen, or uncomfortable around your abdomen can show up when hormones fluctuate, especially in the premenstrual phase. (nhs.uk)
- Worse PMS
- If the week or two before your period feels like a completely different version of you, progesterone may be part of the picture. PMS can include mood symptoms, breast pain, headaches, bloating, irritability, and food cravings. (nhs.uk)
- Mood swings, anxiety, or feeling emotionally less resilient
- Hormonal fluctuations can affect neurotransmitters and sleep, which, in turn, can affect mood. During the menopausal transition, mood changes and anxiety are common enough that NICE specifically recommends considering menopause-focused CBT for some women. (nhs.uk)
- Sleep problems
- You may feel wired at night, wake often, or sleep lightly in the days leading up to your period. Sleep can worsen during times of hormonal change, particularly in perimenopause and menopause. (nhs.uk)
- Headaches or menstrual migraines
- Hormone fluctuations, especially around the late luteal phase and period, can trigger headaches in some women. (nhs.uk)
- Lower libido
- Low progesterone is not the only cause of low desire, but shifting sex hormones, fatigue, stress, sleep loss, and mood changes can all feed into reduced libido. (Cleveland Clinic)
- Irregular ovulation or fertility struggles
- Progesterone rises after ovulation, so if you are not ovulating regularly, progesterone may remain low. That can affect cycle predictability and make conception harder. (Endocrine)
- Symptoms worsening in perimenopause
- For many women, this pattern becomes more obvious in their 40s because ovulation becomes more erratic before periods stop completely. Perimenopause can bring irregular bleeding, breast tenderness, sleep disruption, mood changes, and cycle unpredictability. (acog.org)
What else can look similar?
This is an important Hormone Health point: symptoms that get blamed on “oestrogen dominance” may actually be caused by something else.
Heavy or irregular bleeding can also happen with fibroids, adenomyosis, endometrial polyps, thyroid problems, PCOS, pregnancy-related issues, medication effects, or endometrial changes. Fibroids in particular can cause heavy bleeding, pelvic pain, and pressure symptoms. (acog.org)
That is why we should be cautious about self-diagnosing based solely on social media. A proper history and examination, and sometimes blood tests, cervical screening review, ultrasound, or endometrial assessment, may be needed depending on your age and symptoms. (acog.org)
Hormonal Imbalance in Women: Signs, Causes, and When to Seek Help
Evidence-based solutions
Medical interventions
Treatment depends on your age, symptoms, bleeding pattern, pregnancy plans, medical history, and whether you are in your reproductive years, perimenopause, or menopause.
HRT or prescribed progesterone
If you are in perimenopause or menopause and have symptoms related to falling or fluctuating hormones, HRT may be considered. NHS guidance states that HRT replaces the oestrogen and progesterone that fall during menopause and can help with hot flushes, sleep problems, mood changes, anxiety, and vaginal dryness. (nhs.uk)
For women with a uterus taking systemic oestrogen, a progestogen is usually added to protect the womb lining. Micronised progesterone is one of the prescribed options in some treatment plans. (nhs.uk)
Hormonal contraception
In reproductive-age women, some clinicians may recommend the combined pill, a progestogen-only method, or the levonorgestrel intrauterine system (LNG-IUS), depending on symptoms and contraceptive needs. These options can help regulate bleeding and reduce heavy periods. (acog.org)
Treatment for heavy menstrual bleeding
If heavy bleeding is the main problem, treatment may include:
- hormonal medications
- tranexamic acid or anti-inflammatory medicines in selected cases
- an LNG-IUS
- investigation and treatment of fibroids, polyps, or other underlying causes (acog.org)
Surgery or procedures
If bleeding is severe or linked to structural causes, options may include polyp removal, fibroid procedures, endometrial ablation, or hysterectomy. These are not first-line for everyone, but they can be appropriate in the right clinical context. (acog.org)
A note on supplements and “bioidentical” claims
Be careful with over-the-counter hormone products and heavily marketed supplements. NICE and the Endocrine Society advise caution around custom-compounded hormones, and NCCIH notes that evidence for popular supplements such as black cohosh is inconsistent, with safety concerns including possible liver harm. (Endocrine)

Holistic and lifestyle support
Lifestyle care will not fix every hormone problem, but it can make a meaningful difference to symptoms and overall Hormone Health.
Track your pattern
Keep a simple symptom diary for at least two cycles. Note bleeding, spotting, mood, sleep, headaches, breast symptoms, bloating, and any triggers. NHS guidance specifically recommends symptom tracking for PMS because patterns matter. (nhs.uk)
Support sleep and stress regulation.
Stress does not “cause” every hormone issue, but chronic stress can worsen sleep, anxiety, coping, and cycle symptoms. Gentle nervous system support matters: a consistent bedtime, reduced alcohol close to sleep, therapy, breathing exercises, and realistic workload boundaries can all help. NHS and NICE both recognise stress reduction and CBT as useful symptom support in the right context. (nhs.uk)
Move regularly
Regular physical activity can help with PMS, mood, sleep, and general well-being. It does not need to be extreme. Walking, strength training, yoga, cycling, and swimming all count. (nhs.uk)
Eat in a way that supports stable energy.
A balanced eating pattern with adequate protein, fibre, healthy fats, iron-rich foods if bleeding is heavy, and regular meals can support energy and recovery. Frequent restrictive dieting can make symptoms feel worse for some women, especially when they are already dealing with fatigue and appetite changes.
Cut back on smoking and excess alcohol.
Smoking and heavy alcohol use can worsen symptoms and overall health risk. NHS advice for PMS and menopause support includes reducing alcohol and not smoking. (nhs.uk)
Check for iron deficiency if periods are heavy.
Heavy periods can lead to iron deficiency and anaemia, which can leave you exhausted, breathless, headachy, and foggy. That can easily get mistaken for “just hormones.” Discuss blood testing with your clinician if this sounds familiar. Heavy menstrual bleeding should always be taken seriously. (acog.org)
This is where Hormone Health becomes more than a buzzword. It means looking at the whole picture: bleeding, sleep, mood, nutrition, stress, and medical causes together.
Signs of Endometriosis You Should Not Ignore: Symptoms That Need Attention
When to see a doctor
Please seek medical review if you have any of the following:
- Very heavy bleeding
- Bleeding between periods
- Bleeding after sex
- Any bleeding after menopause
- A sudden major change in your usual cycle
- Pelvic pain, pressure, or abdominal swelling
- Symptoms of anaemia, such as dizziness, breathlessness, palpitations, or extreme fatigue
- A new breast lump or persistent breast change
- Severe low mood, anxiety, or symptoms affecting safety
- Difficulty conceiving or repeated miscarriage
- Unexpected bleeding while on HRT that continues, worsens, or starts after a period of stability (acog.org)
These are not symptoms to self-treat indefinitely with supplements. They need a proper medical assessment.
Frequently Asked Questions
Is oestrogen dominance a real diagnosis?
Not in the formal medical sense. It is a popular term people use to describe symptoms that may relate to unopposed oestrogen effects or low progesterone relative to oestrogen, especially when ovulation is irregular. (The Menopause Consortium)
Can low progesterone cause weight gain?
It may contribute indirectly through bloating, fluid retention, poor sleep, low mood, and appetite changes, but weight changes are rarely explained by a single hormone. A broader review of Hormone Health, lifestyle, thyroid function, and metabolic factors is often more useful. (Cleveland Clinic)
How do doctors test for low progesterone?
Doctors may use your history first: cycle pattern, changes in bleeding, PMS symptoms, fertility history, and age. In some cases, blood tests are timed to the cycle, but testing is not always straightforward because hormone levels fluctuate. Clinical context matters.
Can you have low progesterone in perimenopause?
Yes. Perimenopause often involves more erratic ovulation, which can mean lower or less consistent progesterone production before periods stop altogether. (acog.org)
Will progesterone therapy help everyone?
No. It depends on the cause of your symptoms, whether you are still cycling, whether you need contraception, whether you have a uterus, and whether another diagnosis is present. Treatment should be individualised. (NICE)
Disclaimer
This content is for informational purposes only and does not constitute medical advice.