Perimenopause Brain Fog or ADHD? How to Tell
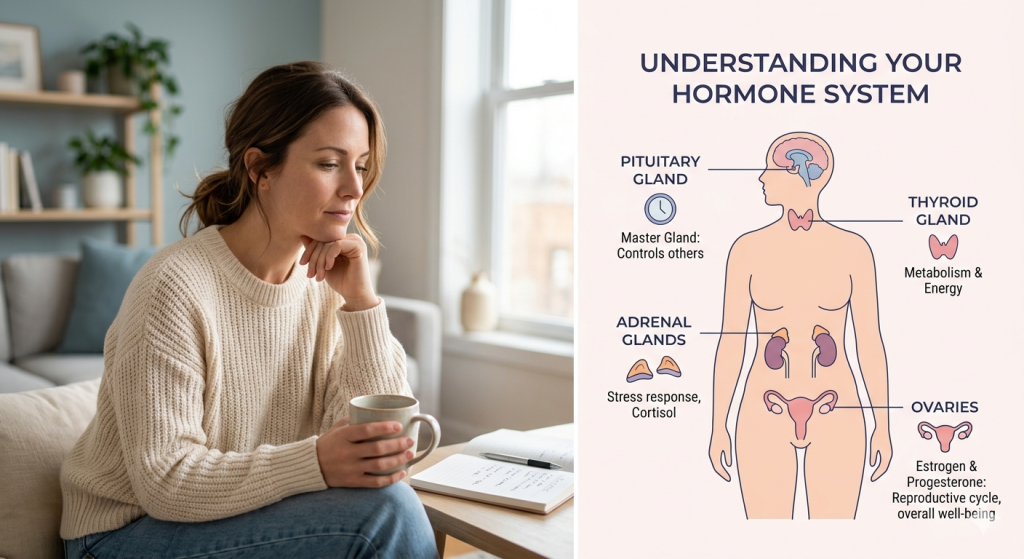
Introduction If you have found yourself standing in the kitchen wondering why you walked in there, rereading the same email three times, forgetting appointments, or feeling mentally “offline,” you are not alone. Many women experience these changes and are seeking answers, which can be reassuring and help them feel understood. Many women start searching for answers when they notice changes in memory, focus, and mental clarity and begin wondering: Is this perimenopause brain fog or ADHD? It can feel unsettling, especially if you have always been organised, capable, and mentally sharp. Some women worry they are developing early dementia. Others wonder if stress is finally catching up with them. And for many women in their late 30s and 40s, hormonal changes during perimenopause may be playing a much bigger role than they realise. Understanding how perimenopause brain fog differs from ADHD is crucial. This article will clarify the unique patterns, helping you distinguish between hormonal changes and lifelong attention difficulties so that you can seek appropriate support. What Is Perimenopause Brain Fog? Perimenopause brain fog is a term used to describe changes in memory, concentration, mental clarity, and processing speed linked to hormonal fluctuations during the years leading up to menopause. It is not a medical diagnosis on its own, but it is a very real symptom experienced by many women during perimenopause. Hormonal shifts, especially changing oestrogen levels, can affect parts of the brain involved in attention, language, mood, and memory. Perimenopause usually begins in a woman’s 40s, although it can start earlier. During this stage, periods may become irregular, and symptoms such as hot flushes, sleep disruption, anxiety, and mood changes often appear. Recognising these as common changes can help women feel more at ease with their experiences. Brain fog can look different from one woman to another. For some, it feels like forgetfulness. For others, it is difficulty concentrating, mental exhaustion, or struggling to multitask as they once did. Quick Answers “Perimenopause brain fog is a collection of memory, focus, and concentration symptoms linked to hormonal changes before menopause.” “Hormonal fluctuations during perimenopause can affect sleep, mood, and cognitive function at the same time.” “ADHD symptoms usually begin earlier in life, while perimenopause brain fog often appears during the late 30s or 40s.” Daily Mood & Hormone Check-In Why Does It Happen? i. Hormonal Changes and the Brain Oestrogen does much more than regulate periods. It also supports brain chemicals involved in memory, mood, focus, and verbal processing. During perimenopause, oestrogen levels fluctuate unpredictably. These hormonal shifts can affect: Attention and concentration Word recall Mental processing speed Sleep quality Emotional regulation Research suggests that sleep disruption and vasomotor symptoms, such as night sweats, may also contribute to cognitive symptoms. You can read more from the British Menopause Society and the NHS menopause guidance. ii. Stress and Mental Overload Midlife is often a time of enormous emotional and mental pressure. Many women are balancing careers, caregiving, parenting teenagers, ageing parents, relationship stress, financial concerns, and chronic exhaustion all at once. Chronic stress increases cortisol levels, which can affect concentration, sleep, and memory. Stress-related cognitive symptoms often include: Feeling mentally overwhelmed Racing thoughts Difficulty switching off Irritability Poor focus during busy or emotional periods iii. Sleep Deprivation Sleep disruption is one of the most overlooked causes of brain fog. Perimenopause commonly affects sleep because of: Night sweats Anxiety Hormonal shifts Frequent waking Insomnia Poor sleep can cause: Forgetfulness Slower thinking Emotional sensitivity Reduced attention span Difficulty finding words iv. Could It Be ADHD? Some women discover ADHD during perimenopause because hormonal changes reduce the brain’s ability to compensate for long-standing attention difficulties. ADHD in women is often missed earlier in life, especially in women who were academically capable or learned to mask symptoms. Signs that ADHD may have been present before perimenopause include: Lifelong disorganisation Chronic procrastination Difficulty completing tasks Emotional impulsivity Time blindness Struggling with focus since childhood or teenage years Perimenopause can sometimes make existing ADHD symptoms feel more intense. The National Institute for Health and Care Excellence (NICE) ADHD guidance provides further information on assessment and diagnosis. Signs and Symptoms Common Symptoms of Perimenopause Brain Fog Forgetting names or words Losing track of conversations Difficulty concentrating Mental fatigue Trouble multitasking Walking into rooms and forgetting why Reduced confidence at work Feeling mentally “slower” Increased anxiety about memory Symptoms are more common in Stress and Burnout Feeling emotionally overwhelmed Constant tension or worry Irritability Difficulty relaxing Trouble focusing during stressful periods Feeling mentally exhausted by decision-making Symptoms Linked to Poor Sleep Waking unrefreshed Daytime sleepiness Poor short-term memory Reduced patience Brain fog that improves after better sleep Symptoms That May Suggest ADHD Lifelong attention difficulties Chronic disorganisation Forgetting deadlines repeatedly Difficulty prioritising tasks Hyperfocus on some tasks but inability to start others Emotional impulsivity Symptoms present before perimenopause What Is Normal and When to Pay Attention? a. Common Changes These symptoms can be common during perimenopause, but are still worth monitoring: Mild forgetfulness Difficulty concentrating during stress Temporary word-finding problems Mental fatigue after poor sleep Feeling less mentally sharp than usual Tracking patterns can help identify triggers. Some women notice symptoms worsen: Before periods During stressful weeks After poor sleep During heavy bleeding or fatigue b. Needs Urgent Attention Please seek medical advice urgently if you experience: Sudden confusion One-sided weakness Difficulty speaking suddenly Severe headaches Fainting Chest pain Shortness of breath Rapid worsening of memory Thoughts of self-harm Major personality changes These symptoms should never automatically be assumed to be perimenopause. Evidence-Based Solutions Treatment depends on the cause, severity, overall health, age, menopause stage, medical history, and personal preferences. Medical Interventions Medical Assessment A healthcare professional may ask about: Menstrual changes Sleep quality Mood symptoms Stress levels Family history Medication use ADHD symptoms in childhood Blood tests may sometimes be used to check: Iron levels Thyroid function Vitamin B12 Vitamin D Anaemia Blood sugar levels Hormone blood tests are not always needed to diagnose perimenopause in women over 45 because symptoms and menstrual changes are
Perimenopause Brain Fog or ADHD? How to Tell Read More »