Introduction
If you are thinking about egg freezing, you are not overthinking it, and you are not late to the conversation. Many of us reach a point where fertility stops feeling like an abstract idea and starts feeling personal, urgent, and tangled up with real life: relationships, career, money, health, and timing.
This guide is here to help us sort through that noise. We will look at what the data actually says about freezing eggs at 30 versus 35, why age matters biologically, what testing can and cannot tell us, what the process involves, and how to make a decision that feels informed rather than fear-driven. The short version is this: for most women, 30 gives better odds than 35, but 35 can still be a very reasonable and worthwhile age to freeze eggs, especially if you may need more than one cycle or you are not ready to try for pregnancy yet. (ASRM)
What this guide will help you understand
When people ask whether 30 or 35 is the best age to freeze eggs, they are usually asking something deeper:
-
Will waiting 5 years meaningfully change my odds?
-
Am I too early to do this now?
-
Am I already cutting it close?
-
Will egg freezing actually protect my future fertility?
Those are sensible questions. The evidence suggests that age at the time the eggs are frozen matters more than age at the time the eggs are used later. Eggs frozen younger generally have a better chance of leading to a baby because both egg number and egg quality decline with age, and this decline becomes more noticeable in the mid-30s and steeper after the late 30s. (HFEA)
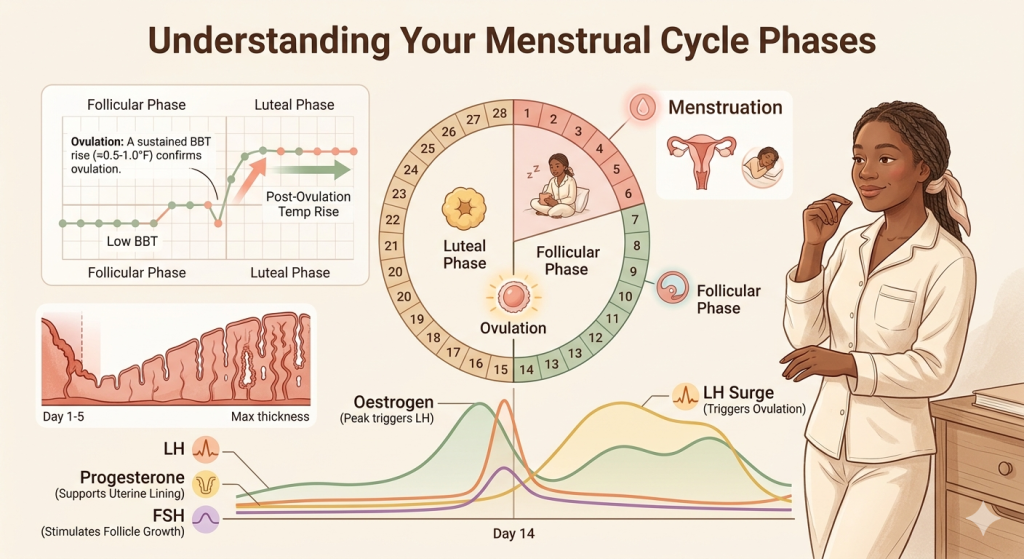
Why age matters so much in fertility and egg freezing
a) The biology, in plain language
We are born with all the eggs we will ever have. Over time, that egg supply naturally gets smaller. But it is not only about quantity. As we get older, a larger share of eggs are more likely to have chromosomal problems, which makes fertilisation, embryo development, implantation, and miscarriage outcomes less favourable. (PubMed)
That is why fertility changes with age, even in healthy women with regular periods. Regular cycles can indicate that ovulation is occurring, but they do not guarantee that egg quality has remained the same. Professional guidance consistently notes that female fertility declines gradually beginning in the early 30s, becomes more noticeable after 35, and drops more rapidly later in the decade. (PubMed)
b) Why does that matter for egg freezing
Egg freezing preserves eggs at the age they are collected. In other words, if eggs are frozen at 30 and used at 40, they are still biologically 30-year-old eggs. That is the central reason age at freezing is so important. HFEA guidance specifically notes that success is more strongly linked to the age at which the eggs were frozen than to the age at which they are thawed and used. (HFEA)
Is 30 or 35 the better age to freeze eggs?
The evidence-based answer
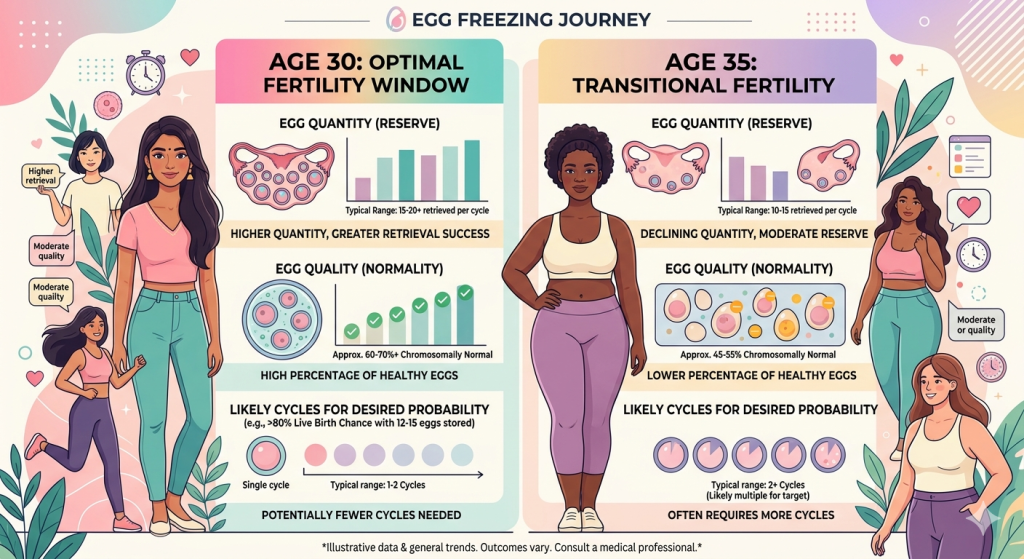
For most women, 30 is biologically the better age to freeze eggs because:
-
You are more likely to retrieve more eggs in one cycle.
-
A higher proportion of those eggs is likely to be mature and chromosomally normal.
-
You may need fewer cycles to reach a useful target number of frozen mature eggs.
A recent age-based study of elective egg freezing found that at the 50th percentile, women aged 30 retrieved about 20 total oocytes and froze around 15 mature eggs, while women aged 35 retrieved about 14 total oocytes and froze around 11 mature eggs. That difference matters because future live birth odds rise with both younger age and more mature eggs banked. (PMC)
ASRM’s evidence summary cites modelling suggesting that to reach about a 70% chance of a live birth, women aged 30–34 may need around 14 mature oocytes, while women aged 35–37 may need around 15. On paper, that sounds similar, but the practical difference is that women at 35 often retrieve fewer mature eggs per cycle than women at 30, so they may be more likely to need another round. (ASRM)
So does that mean 35 is “too late”?
No. Thirty-five is not too late. It is just not as favourable as 30. In real-world practice, many women freeze eggs around 35, and it can still be a smart fertility-preserving choice. HFEA reports that the average age of egg freezing patients in the UK was 35 in 2023. (HFEA)
The better framing is this:
-
If you are deciding between 30 and 35, and all else is equal, 30 is better.
-
If you are already 35 and considering freezing, that does not mean you have missed your chance.
-
If you wait from 30 to 35, you may reduce efficiency and increase the number of cycles needed.
That is why many experts talk about the “best” age clinically as under 35, while acknowledging that the “right” age personally depends on your life, ovarian response, finances, and whether pregnancy is realistically likely in the near future. (Cambridge University Hospitals)
What the numbers say: egg yield, quality, and future live birth chances
1. Egg number falls with age
The more mature eggs you freeze, the better your chances later, because not every egg survives thawing, fertilises, develops into a usable embryo, implants, or results in a live birth. That is normal biology, not failure. (OUP Academic)
A 2017 counselling model found that the probability of at least one live birth rises with the number of mature eggs frozen and is consistently better at younger ages. (OUP Academic)
2. Egg quality also changes with age
This is the part many people feel, but that is not always clearly explained. You can still ovulate regularly at 35, but the chance that an egg has normal chromosomes is lower than it was at 30. That is one reason miscarriage risk also increases with age. (ESHRE)
3. Egg freezing is helpful, but not a guarantee
ASRM states that planned oocyte cryopreservation is ethically permissible and may help avoid future infertility, but patients should also understand the uncertainties and limitations. Egg freezing improves future options; it does not guarantee a baby. (ASRM)
4. Ovarian reserve tests are useful, but limited
AMH and antral follicle count can help estimate how your ovaries may respond to stimulation, which matters for egg freezing planning. But they do not reliably predict your chance of natural conception on their own. Age remains the most important single factor in counselling. (ASRM)
Signs you may be thinking about egg freezing
You may not have “symptoms” in a disease sense, but there are very real signs that this decision is weighing on you. You might be:
- Feeling anxious that your fertility window may be narrowing
- Unsure whether you want children, but not comfortable losing the option
- In a relationship that is not yet ready for parenthood
- Single and worried that timing may be dictated by circumstances rather than choice
- Aware of a family history of early menopause or reduced ovarian reserve
- Planning medical treatment that could affect fertility, such as chemotherapy or pelvic surgery
- Feeling torn between career timing, finances, health goals, and family planning
- Wanting a concrete plan instead of carrying low-grade uncertainty every month
These feelings are common, and they deserve thoughtful support rather than pressure.
What egg freezing can and cannot do
1. What it can do
Egg freezing can:
-
Preserve eggs at your current age.
-
It could potentially reduce the impact of age-related fertility decline later.
-
Give more reproductive flexibility if pregnancy is not likely soon.
-
It is especially useful before medical treatment that may harm the ovaries.
Professional guidance from ESHRE supports vitrified oocyte cryopreservation as the method of choice for many women seeking fertility preservation. (OUP Academic)
2. What it cannot do
Egg freezing cannot:
-
Stop the rest of your reproductive system from ageing.
-
Guarantee a future pregnancy or live birth.
-
Fully offset all age-related pregnancy risks later in life.
-
Promise you will only need one cycle.
That nuance matters. Freezing eggs preserves egg age, but not the uterus’s age, nor broader health factors that can affect pregnancy at 40 or 42. (ASRM)
Medical options and fertility-preserving interventions
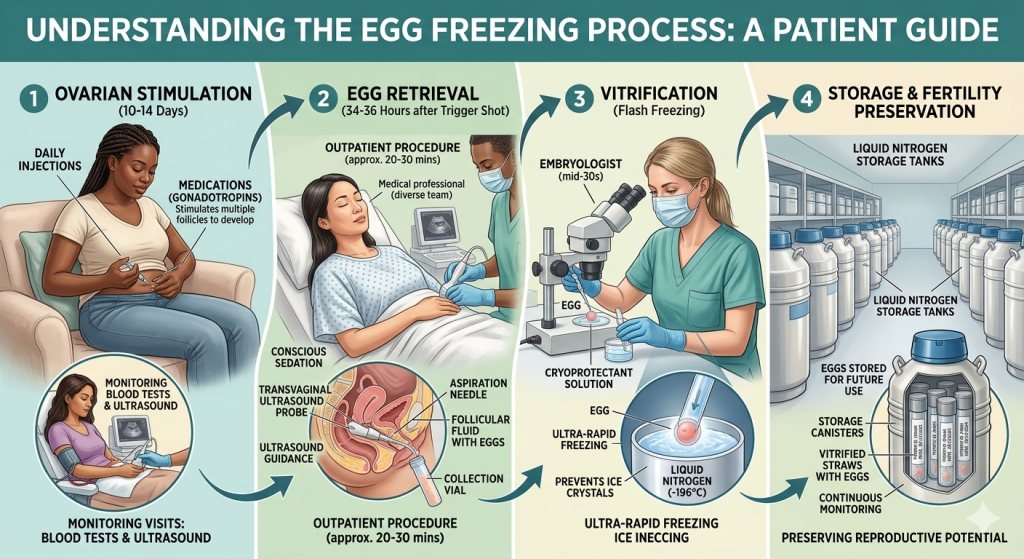
1. Planned egg freezing
This is the main medical intervention for someone trying to preserve future fertility for age-related reasons. It involves ovarian stimulation with injectable hormones, ultrasound and blood monitoring, and a short procedure to retrieve eggs, which are then vitrified and stored. (ESHRE)
2. Embryo freezing
For women with a partner or donor sperm and a clear plan, embryo freezing may be another option. Some patients prefer it because embryos may provide different planning information later, but it is a more committed path than freezing unfertilised eggs. (ESHRE)
3. Ovarian reserve testing before treatment
A fertility specialist will often check:
-
AMH
-
Antral follicle count
-
Baseline ultrasound
-
Sometimes, day-3 hormones, depending on the clinic
These tests help predict response to stimulation, not your absolute future fertility. (ASRM)
4. Risk management during treatment
Egg freezing is generally safe, but there are risks. The most important treatment-related complication is ovarian hyperstimulation syndrome (OHSS). Severe OHSS is now rare, but symptoms can include worsening abdominal swelling, nausea, vomiting, shortness of breath, reduced urine output, and severe pain. Rare procedural risks include bleeding, infection, and bowel perforation. (HFEA)

Holistic and lifestyle support for fertility
Lifestyle cannot “reverse” egg ageing, and it is important to say that plainly. But it can support overall reproductive health, treatment readiness, and pregnancy outcomes.
a. Nutrition
Aim for a balanced pattern built around:
- Adequate protein
- Fibre-rich carbohydrates
- Unsaturated fats
- Iron-rich foods
- Folate-containing foods
Before treatment or pregnancy, most women are advised to take folic acid. Your clinician may recommend other supplements based on your risk of deficiencies, diet, or lab results. (ESHRE)
b. Exercise
Regular moderate activity supports metabolic health, stress regulation, and sleep. Extreme exercise or under-fueling can negatively affect ovulation in some women, so balance matters.
c. Smoking, alcohol, and substance use
Smoking is linked with earlier reproductive decline and poorer fertility outcomes. Reducing or stopping smoking is one of the clearest evidence-based changes you can make for reproductive health. (ESHRE)
d. Sleep and stress
Stress does not directly “use up” your eggs, but chronic stress can make decision-making, treatment, recovery, and emotional well-being much harder. Therapy, coaching, mindfulness, journaling, and support groups can all help.
e. Weight and metabolic health
Being significantly underweight or living with unmanaged metabolic conditions can affect ovulation and treatment planning. This is not about blame. It is about creating the best possible conditions for your body before a medical intervention.
When to see a doctor
If egg freezing is on your mind, you do not need to wait for a crisis. A consultation can be useful if you are trying to make a sound decision about your fertility.
Book a fertility consultation if:
- You are deciding between freezing now versus waiting a few years
- You are 35 or older and want realistic counselling about timing
- You have irregular or absent periods
- You have endometriosis, PCOS, prior ovarian surgery, or pelvic inflammatory disease
- You have a family history of early menopause
- You are planning chemotherapy, radiation, or surgery that may affect the ovaries
- You have been trying to conceive for 6 months if you are over 35
- You have been trying to conceive for 12 months if you are under 35
ASRM and older age-related fertility guidance support earlier fertility evaluation after 6 months of trying in women over 35. (PubMed)
Red flag symptoms: seek urgent medical review if you have
- Severe pelvic or abdominal pain during or after stimulation
- Rapid abdominal swelling
- Shortness of breath
- Fainting or chest pain
- Heavy vaginal bleeding
- Fever after egg retrieval
- Very reduced urine output
- Persistent vomiting
These can suggest OHSS or another complication and should not be ignored. (RCOG)
Frequently Ask Questions
Q: Is 30 or 35 the best age to freeze eggs?
A: Thirty is usually better biologically than 35 because both egg quantity and egg quality are generally stronger, and you may retrieve more mature eggs in one cycle. But 35 is still often a good age to freeze eggs, especially if pregnancy is not likely soon. (PMC)
Q: Is 35 too old to freeze your eggs?
A: No. Thirty-five is not too old. Outcomes are usually better under 35, but many women still freeze eggs at 35 and later. The question is less “too old” and more “how efficient is it likely to be, and how many cycles might I need?” (HFEA)
Q: How many eggs should I freeze for one baby?
A: There is no magic number, but models cited by ASRM suggest that about 14 mature oocytes at ages 30–34 and about 15 at ages 35–37 correspond to about a 70% chance of a live birth. Real outcomes vary by clinic, egg survival, sperm factors, embryo development, and uterine factors. (ASRM)
Q: Does AMH tell me if I should freeze my eggs?
A: Not by itself. AMH helps estimate ovarian response to stimulation, which is useful for planning egg freezing, but it does not reliably predict your natural fertility on its own. (ASRM)
Q: Is egg freezing a guarantee against infertility?
A: No. Egg freezing can improve future reproductive options, but it does not guarantee pregnancy or live birth. It is best understood as a way to preserve possibility rather than promise. (ASRM)
Q: Does egg freezing protect fertility forever?
A: It preserves eggs at the age they were frozen, but it does not guarantee future pregnancy or remove all age-related pregnancy risks later.
Q: Can AMH predict my future fertility?
A: AMH can help estimate how the ovaries may respond during egg freezing, but it does not reliably predict your chance of natural conception on its own.
Q: When should I see a fertility doctor?
A: See a fertility specialist if you are 35 or older and weighing timing decisions, have irregular cycles, have risk factors such as endometriosis or ovarian surgery, or are planning treatment that may harm fertility.
Final takeaway
If we are choosing strictly between 30 and 35, the medical evidence clearly favours 30 for egg freezing. You are more likely to get more mature eggs, and those eggs are more likely to be of better quality. That usually means better efficiency and fewer cycles. (PMC)
But life is rarely that neat. For many women, 35 is still a good and reasonable age to preserve fertility, and it is definitely worth doing if the alternative is waiting longer. The best decision is not always the youngest possible one. It is the one that honestly balances biology, timing, finances, emotional readiness, and your real life. (HFEA)
Disclaimer: This content is for informational purposes only and does not constitute medical advice.