The Overview
There is a particular kind of anger that can arrive in perimenopause and feel nothing like your usual self. It may come fast. It may feel disproportionate. It may leave you thinking, Why did I react like that? And then, because women are so often trained to manage everyone else’s comfort, the anger is quickly followed by guilt.
Hormones and anger are not about blaming every feeling on oestrogen or pretending hormones explain everything. It is about understanding that perimenopause can change the biological conditions your brain uses to regulate emotion.
Perimenopause is the transition leading up to menopause, when ovarian hormones fluctuate before periods eventually stop. Menopause itself is confirmed after 12 months without a period. During this transition, many women experience changes in sleep, temperature control, periods, weight distribution, libido, memory, concentration, anxiety, low mood, and emotional steadiness. The NHS recognises mood swings, low mood, depression, memory problems, and concentration changes as symptoms of perimenopause and menopause, and notes that these can feel worse when sleep is poor and exhaustion builds. (nhs.uk)
So no, you are not “just angry.” You may be under-slept, hormonally sensitive, overloaded, inflamed by stress, carrying invisible labour, and trying to function in a body whose internal settings are shifting.
That does not mean anger is harmless or that we should ignore its impact on relationships, work, parenting, or self-esteem. It means anger deserves context, care, and a plan — not shame.
Menopause Mood Tracker Tool
The In-Depth Study
What emotional regulation mean
Emotional regulation means your ability to notice, tolerate, express, and recover from emotions without being completely taken over by them. It is not the same as never feeling angry. Healthy emotional regulation allows you to feel anger, understand what it is signalling, and respond rather than explode, freeze, withdraw, or spiral.
During perimenopause, emotional regulation may become harder because several systems are changing at once: reproductive hormones, sleep, stress response, metabolism, brain chemistry, and life demands.
Why oestrogen matters for mood
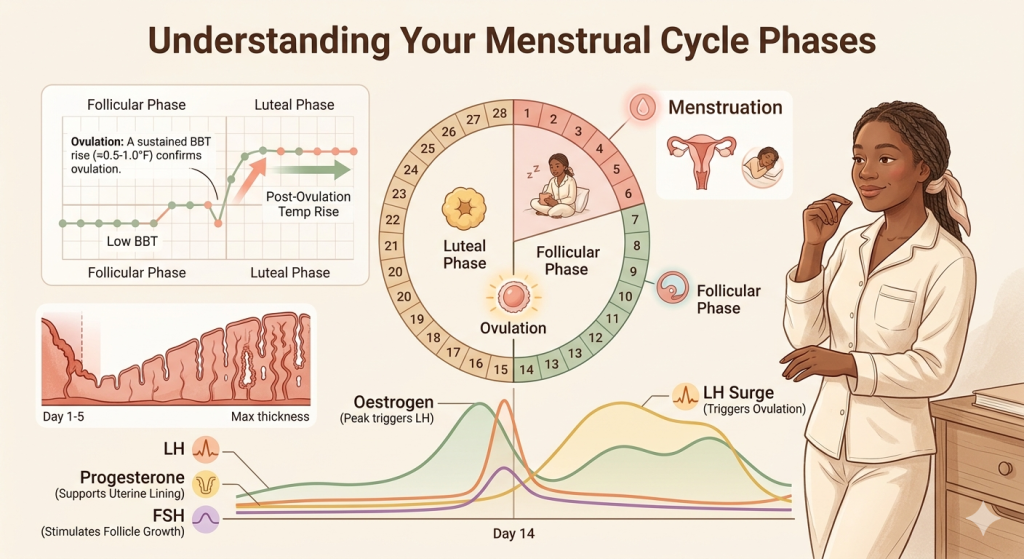
Oestrogen is not only a reproductive hormone. It also interacts with brain systems involved in mood, sleep, cognition, temperature regulation, and stress sensitivity. During perimenopause, oestrogen can rise and fall unpredictably rather than decline in a straight line. That instability can be harder for some women than a steady low level.
Research continues to explore how oestrogen affects neurotransmitters — chemical messengers such as serotonin, dopamine, and noradrenaline — which influence mood, motivation, reward, focus, and emotional sensitivity. A 2025 review on perimenopausal depression describes oestrogen’s role in mood-related brain pathways and why hormonal fluctuation may contribute to depressive and emotional symptoms in susceptible women. (PMC)
This is one reason Hormones and Anger can feel so personal. Your usual coping tools may still be there, but the threshold for overwhelm may be lower.
Progesterone, calm, and the “short fuse”
Progesterone is often described as a calming hormone because some of its metabolites interact with GABA, a brain system involved in relaxation and inhibition. In perimenopause, progesterone may decline earlier or become less consistent, especially as ovulation becomes irregular.
For some women, this can feel like losing an internal buffer. Things that once rolled off your back may suddenly land hard. Noise, mess, interruptions, unfairness, being touched out, being dismissed, or carrying too much responsibility can trigger anger faster than before.
That anger is not imaginary. It is often a signal that your nervous system is running with less reserve.
Sleep disruption makes anger louder
Perimenopause-related insomnia, night sweats, early waking, and restless sleep can make emotional regulation much harder. Poor sleep affects the prefrontal cortex — the part of the brain involved in judgement, impulse control, perspective, and decision-making — while increasing reactivity in threat-detection systems.
In plain English: when you are sleeping badly, your brain has less space between trigger and reaction.
NICE recommends discussing management options based on individual symptoms and circumstances. It includes menopause-specific cognitive behavioural therapy as an option for vasomotor symptoms such as hot flushes and night sweats, either alongside HRT, when HRT is contraindicated, or when someone prefers not to use HRT. (NICE)
Anger is often the visible tip of a bigger symptom cluster
Many women search for hormones and anger because anger is the symptom that scares them most. But underneath it, there may be:
- 3 a.m. waking
- night sweats
- anxiety
- low mood
- brain fog
- migraines
- heavier or irregular periods
- palpitations
- low libido
- relationship strain
- workplace stress
- caring responsibilities
- blood sugar dips
- burnout
This matters because treatment works best when the whole pattern is seen, not just the loudest symptom.
Signs and Symptoms
a. Emotional signs to watch for
Perimenopause-related anger may show up as:
- feeling suddenly irritable or impatient
- snapping over small things
- rage that feels out of proportion
- crying after anger
- feeling overstimulated by noise, clutter, touch, or demands
- intense frustration before or during periods
- feeling less emotionally resilient than usual
- shame after conflict
- withdrawing because you are afraid of your own reactions
The Office on Women’s Health lists mood changes among common menopause-related symptoms and encourages personalised symptom management plans, which is important because emotional symptoms rarely happen in isolation. (Office on Women’s Health)
b. Physical symptoms that may travel with anger
Anger may rise alongside physical changes such as:
- hot flashes or night sweats
- poor sleep
- headaches or worsening migraines
- breast tenderness
- joint aches
- palpitations
- heavier, lighter, closer, or skipped periods
- weight gain around the abdomen
- vaginal dryness or urinary symptoms
The NHS notes that perimenopause and menopause can include mood changes, memory and concentration problems, weight changes, urinary symptoms, headaches, palpitations, joint pains, skin changes, and reduced libido. (nhs.uk)
When anger may be more than perimenopause
Perimenopause can contribute to emotional dysregulation, but it should not be used to explain away everything. Speak with a healthcare professional if anger is:
- new, intense, or worsening
- linked with panic attacks or depression
- affecting your relationships, work, parenting, or safety
- connected to trauma triggers
- accompanied by heavy alcohol use or substance use
- associated with thoughts of self-harm or not wanting to be here
- happening with severe insomnia
- accompanied by unusually high energy, impulsivity, risky behaviour, or reduced need for sleep
Seek urgent help if you feel at risk of harming yourself or someone else.
A note on medical advocacy
Many women are told they are “too young,” “just stressed,” or “probably depressed” without anyone asking about their cycle, sleep, hot flashes, night sweats, libido, vaginal symptoms, migraines, or family history. NICE states that menopause and perimenopause are usually identified through clinical history and symptoms, and advises against using several hormone tests to identify perimenopause or menopause in people aged 45 or over. (NICE)
Bring a symptom diary. Track your cycle if you still have periods. Write down sleep, anger episodes, hot flashes, night sweats, bleeding changes, stress load, and any triggers. You deserve to be assessed as a whole person.
Why Am I Waking at 3 A.M. in Perimenopause?
Diagnosis and Treatment
How clinicians assess perimenopause-related mood changes
There is no single “anger blood test.” A good assessment usually includes:
- age and menstrual pattern
- cycle changes
- sleep quality
- vasomotor symptoms, such as hot flashes and night sweats
- mood history, including PMS, PMDD, depression, anxiety, trauma, postnatal mood changes
- current stressors and caring load
- medication review
- thyroid symptoms
- alcohol, caffeine, and substance use
- relationship safety
- risk assessment for self-harm or harm to others
Depending on your symptoms, your clinician may check thyroid function, iron levels, B12, vitamin D, glucose/HbA1c, or other markers. These do not “diagnose anger,” but they can identify other contributors to fatigue, anxiety, palpitations, low mood, and poor resilience.
Hormone therapy: where it may fit
Hormone replacement therapy, or HRT, replaces oestrogen and, for people with a uterus, usually includes a progestogen to protect the womb lining. NICE recommends offering HRT for vasomotor symptoms associated with menopause and tailoring the discussion of benefits and risks to the person’s age, circumstances, and risk factors. (NICE)
HRT may help with emotional symptoms indirectly by reducing hot flashes, night sweats, and sleep disturbances. Some women also report a more stable mood when hormonal fluctuation is better managed. However, HRT is not a universal cure for anger, and it may not be suitable for everyone.
You may need specialist advice if you have a personal history of breast cancer, blood clots, stroke, coronary heart disease, complex migraine, liver disease, unexplained vaginal bleeding, or other risk factors.
Antidepressants and mental health treatment
If symptoms meet criteria for depression, anxiety, PMDD, trauma-related distress, or another mental health condition, treatment may include psychological therapy, antidepressant medication, or both. SSRIs and SNRIs can be helpful for some mood symptoms and may also reduce hot flashes in some people.
This does not mean “it is all in your head.” Mental health care and menopause care can work together.
CBT and nervous system tools
Cognitive behavioural therapy, or CBT, helps people understand links between thoughts, feelings, body sensations, and behaviours. Menopause-specific CBT may include sleep strategies, hot flash coping skills, stress management, and reframing fear around symptoms. The British Menopause Society lists CBT for menopausal symptoms and sleep disturbance guidance among its clinician resources. (British Menopause Society)
CBT is not about telling women to tolerate poor care or “think positive.” Used well, it gives practical tools for moments when the nervous system is already activated.
Barriers and Challenges
“I don’t recognise myself”
One of the hardest parts of Hormones and Anger is identity shock. You may have spent years being calm, capable, patient, nurturing, or composed. Then suddenly you feel reactive, resentful, blunt, tearful, or easily overwhelmed.
That can be frightening, especially for women who work in caring roles, leadership, parenting, teaching, healthcare, or emotionally demanding jobs.
Shame keeps women quiet
Many women will talk about hot flashes before they admit to rage. Anger can feel socially unacceptable, especially for women expected to be endlessly gentle. But silence makes symptoms harder to treat.
You are allowed to say:
“I am more irritable than usual, and it is affecting my life.”
That is a valid clinical concern.
Misdiagnosis and missed context
Perimenopause can overlap with depression, anxiety, ADHD, thyroid disease, burnout, trauma, medication side effects, relationship stress, and sleep disorders. The overlap is real. The mistake is assuming only one explanation is possible.
A woman can be perimenopausal and depressed. She can have ADHD and worsening hormonal sensitivity. She can be burnt out and hormonally vulnerable. She may need HRT and therapy. She may need rest and medical investigation.
Access and equity
Not every woman receives the same menopause care. Women from ethnic minority backgrounds, women with disabilities, LGBTQ+ people, women with early menopause, people with complex medical histories, and those who are dismissed because they still have periods may face extra barriers. NICE specifically notes that people from some ethnic minority backgrounds and people with some lifelong conditions may experience menopause at a younger age. (NICE)
Good care should be individualised, culturally aware, and safe.
Solutions and Support
Step 1: Track the pattern, not just the explosion For two to four weeks, track:
- anger intensity from 1–10
- sleep length and quality
- night sweats or hot flashes
- period timing
- caffeine and alcohol
- skipped meals or blood sugar dips
- conflict triggers
- workload and caring load
- physical symptoms
- what helped you recover
This helps you move from self-blame to pattern recognition.
Step 2: Build a “pause plan” for anger surges
When anger rises, your body needs interruption before insight. Try:
- stepping away for 90 seconds
- unclenching jaw and hands
- cooling the body with water, fan, open window, or cool cloth
- saying, “I need a moment. I will come back to this.”
- lowering noise and stimulation
- eating protein if you have not eaten
- writing the sentence you want to say before saying it
This is not avoidance. It is nervous system first aid.
Step 3: Protect sleep like treatment
Sleep is not a luxury in perimenopause. It is emotional regulation medicine.
Helpful starting points include:
- consistent wake time
- cool bedroom
- reducing alcohol near bedtime
- limiting late caffeine
- light exposure in the morning
- winding down before bed
- addressing night sweats medically if they are frequent
- discussing insomnia treatment if sleep remains poor
Step 4: Stabilise blood sugar and energy
Blood sugar dips can intensify irritability, anxiety, shakiness, and anger. Aim for regular meals with protein, fibre, and healthy fats. This is especially important if you are skipping meals, dieting aggressively, fasting, or living on caffeine during stressful days.
No supplement “cures” perimenopause anger. But a consistent food rhythm, adequate hydration, and enough protein can reduce the number of avoidable triggers your nervous system has to handle.
Step 5: Move emotion through the body
Exercise supports mood, sleep, insulin sensitivity, bone health, cardiovascular health, and stress regulation. You do not need punishing workouts. Walking, strength training, yoga, swimming, dancing, cycling, or short movement breaks can help.
The goal is not to “burn off rage” as punishment. The goal is to give stress somewhere to go.
Step 6: Consider clinical options
Depending on your history and symptoms, support may include:
- HRT
- menopause-specific CBT
- treatment for depression or anxiety
- sleep treatment
- review of contraception
- treatment for heavy bleeding
- vaginal oestrogen for genitourinary symptoms
- migraine management
- thyroid or iron treatment if abnormal
- workplace adjustments
- relationship or family support
The 2025 European Society of Endocrinology guideline covers evaluation and management of menopause and perimenopause, including hormonal and non-hormonal therapies, and highlights the importance of individualised care for women with different risk profiles. (OUP Academic)
Step 7: Repair without self-erasure
If anger has affected someone else, repair matters. But repair does not require self-hatred.
Try:
“I’m sorry I shouted. That wasn’t okay. I’m also realising my symptoms are getting harder to manage, and I’m going to get support. I need us to talk about what I’m carrying before I reach breaking point.”
Accountability and compassion can exist in the same sentence.
Conclusion
Hormones and anger are not a character flaw. It is often a sign that your emotional regulation system is under pressure from hormonal fluctuation, poor sleep, stress, physical symptoms, and life load.
Perimenopause can make the margin between “I’m fine” and “I cannot cope with one more thing” much thinner. The answer is not to shame yourself into silence. The answer is to understand the pattern, protect your nervous system, seek medical support when symptoms interfere with life, and build a care plan that treats you as a whole person.
Your anger may be asking for rest. It may be asking for boundaries. It may be asking for oestrogen support, therapy, sleep treatment, food rhythm, less invisible labour, or a clinician who knows how to listen.
Most of all, it is asking not to be dismissed.
Takeaway
Summary box: What to do next
- Name it without shame: “My anger has changed, and I want to understand why.”
- Track your pattern: cycle, sleep, hot flashes, food, stress, anger triggers, and recovery time.
- Prioritise sleep: poor sleep lowers emotional tolerance.
- Book a menopause-informed review, especially if symptoms are new, worsening, or affecting relationships or work.
- Ask about options: HRT, CBT, antidepressants, sleep support, contraception, and treatment for related symptoms.
- Check safety: seek urgent help if you feel at risk of harming yourself or someone else.
- Use FemPhases tools: Not sure where your symptoms fit? Take the Tools and Quizzes to understand your pattern.
Frequently Asked Questions
1. Can perimenopause cause anger?
Yes, perimenopause can contribute to anger, irritability, mood swings, and emotional sensitivity. Hormone fluctuation, poor sleep, hot flashes, stress, and life load can all lower emotional resilience.
2. Why do I feel rage before my period in my 40s?
Hormonal shifts can become more unpredictable in perimenopause. If progesterone is lower or ovulation is irregular, some women feel more premenstrual irritability, anxiety, or rage than they did before.
3. Is perimenopause anger the same as depression?
Not always. Anger can appear on its own, but it can also be part of depression, anxiety, PMDD, trauma, burnout, or sleep deprivation. If anger is persistent, intense, or affecting your life, speak with a healthcare professional.
4. Will HRT help with anger and mood swings?
HRT may help some women, especially when mood symptoms are linked with hot flashes, night sweats, and poor sleep. It is not suitable for everyone and is not the only option, so decisions should be individualised.
5. What can I do in the moment when anger suddenly spikes?
Pause before responding. Step away, cool your body, breathe slowly, drink water, reduce stimulation, and use a simple phrase such as “I need a moment before I answer.” Return to the conversation when your body has settled.
6. When should I seek urgent help for anger?
Seek urgent support if you feel you might harm yourself or someone else, if you feel out of control, if anger comes with suicidal thoughts, or if you have extreme mood changes with risky behaviour or reduced need for sleep.
7. Can lifestyle changes really help with perimenopause mood swings?
Yes, but they should not be used to dismiss medical care. Sleep support, regular meals, movement, reduced alcohol intake, stress management, and boundaries can support emotional regulation. Some women also need HRT, therapy, or medication.
Medical Disclaimer
This article is for educational purposes only and does not replace personalised medical advice, diagnosis, or treatment. If you are worried about your symptoms, if your symptoms are getting worse, or if something does not feel right in your body, please speak with your doctor, nurse practitioner, gynaecologist, endocrinologist, or another qualified healthcare professional. Seek urgent medical help for severe, sudden, or concerning symptoms.