Introduction
Somewhere between the hot flashes, the stubborn belly fat, the 3 a.m. waking, and the feeling that your body has quietly changed the rules, it makes sense that women are asking about GLP-1 microdosing in perimenopause. Not because they are vain. Not because they lack discipline. But because many are tired of being told that symptoms disrupting their daily lives are just “normal ageing.”
GLP-1 medicines, such as semaglutide and tirzepatide, have changed the conversation around obesity, type 2 diabetes, appetite regulation, and metabolic health. The NHS describes semaglutide as a prescription GLP-1 agonist used to manage type 2 diabetes or treat obesity alongside diet and exercise changes. (nhs.uk)
But GLP-1 microdosing in perimenopause is a different conversation. It sits in a grey zone between medical treatment, off-label prescribing, social media trends, and private wellness marketing. The key question is not “Could GLP-1 medicines help some women?” They can, when clinically appropriate. The better question is: Is microdosing evidence-based, safe, and appropriate for your body right now?
Menopause Symptom Checker Quiz
The Overview
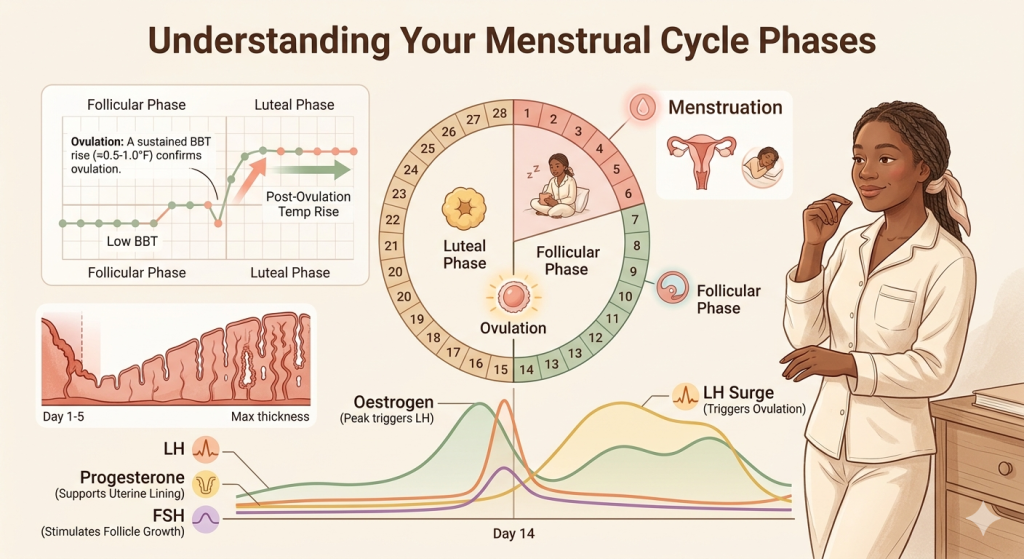
Perimenopause is the transition leading up to menopause, when ovarian hormone patterns become more unpredictable. Oestrogen and progesterone may rise and fall unevenly before periods stop completely. For many women, this stage brings hot flashes, night sweats, heavier or irregular periods, sleep disturbance, anxiety, joint aches, brain fog, and changes in body composition.
At the same time, midlife metabolism can feel less forgiving. Muscle mass may decline, sleep disruption can affect hunger hormones, stress can increase cravings, and changing oestrogen levels may influence fat storage around the abdomen. This does not mean weight gain is inevitable. It does mean that the old advice to “eat less and move more” can feel painfully incomplete.
GLP-1 microdosing in perimenopause has grown from this frustration. The idea is usually to use a lower-than-standard dose of a GLP-1 medicine to reduce appetite, improve cravings, support blood sugar stability, or avoid the stronger side effects some people experience at standard doses.
However, there is an important distinction:
Clinician-guided dose adjustment is not the same as wellness “microdosing.” A prescriber may adjust a medication carefully due to side effects, treatment response, medical history, or tolerability. But the current microdosing trend often involves non-standard doses, compounded products, online prescribing, or vague claims about “longevity,” “inflammation,” or “hormone balancing.”
As of 2026, medical caution is warranted. STAT reported that there is no agreed clinical definition of GLP-1 microdosing for weight loss and no legitimate long-term evidence supporting it as a treatment approach. (STAT)
The In-Depth Study
What are GLP-1 medicines?
GLP-1 stands for glucagon-like peptide-1, a hormone involved in appetite, digestion, insulin release, and blood sugar control. GLP-1 receptor agonists are medicines that mimic this hormone.
In plain English, they can help some people:
- Feel fuller for longer
- Have fewer intense food cravings
- Lower blood sugar levels
- Lose weight when used alongside nutrition, movement, and medical supervision
- Improve some obesity-related cardiometabolic risks
The World Health Organisation’s 2025 guidance describes GLP-1 receptor agonists as medicines that can lower blood sugar, support weight loss, reduce the risk of certain heart and kidney complications, and reduce the risk of early death in people with type 2 diabetes. Its obesity guidance focuses on liraglutide, semaglutide, and tirzepatide. (World Health Organisation)
What does “microdosing” mean?
This is where things get slippery.
In medicine, dosing should be precise: a drug, a dose, a schedule, a reason, a monitoring plan, and clear safety instructions. But GLP-1 microdosing in perimenopause does not yet have a standard medical definition.
Depending on who is using the term, it may mean:
- Starting at the lowest licensed dose and staying there longer
- Taking a fraction of a standard dose
- Spacing injections further apart
- Using compounded semaglutide or tirzepatide
- Using GLP-1s for mild weight gain, cravings, “metabolic optimisation,” or longevity
- Using the medication without meeting formal obesity, diabetes, or cardiometabolic criteria
That lack of clarity matters. Without a shared definition, it is difficult to study safety, effectiveness, side effects, dose-response, or long-term outcomes.
Why are perimenopausal women interested
The interest is understandable. Many women in their 40s and 50s are dealing with symptoms that overlap: poor sleep, higher stress, increased abdominal fat, stronger cravings, fatigue, low mood, and reduced exercise recovery.
Some women also develop insulin resistance, meaning the body has a harder time using insulin effectively to move glucose from the blood into cells. This can contribute to hunger, weight gain, raised blood sugar, and higher cardiometabolic risk.
But perimenopause is not one single problem. Stubborn weight gain may be linked to sleep deprivation, thyroid disease, polycystic ovary syndrome, medication side effects, depression, stress, reduced muscle mass, alcohol intake, insulin resistance, or untreated menopause symptoms. That is why GLP-1 microdosing in perimenopause should not be used as a shortcut around proper assessment.
What does the evidence say so far?
The strongest evidence for GLP-1 medicines is in people with type 2 diabetes, obesity, overweight with weight-related complications, and some cardiovascular risk groups. NHS England states that semaglutide for obesity is prescribed through specialist weight management services and may be considered when diet and exercise changes have not worked on their own. (NHS England)
For menopause specifically, the research is still developing. The British Menopause Society published a 2025 clinician tool on incretin-based therapies, including GLP-1 medicines, in women using HRT. The guidance highlights indications, menopause-related prescribing considerations, and clinical practice guidance. (British Menopause Society)
But GLP-1 microdosing in perimenopause is not yet backed by robust long-term trials. That does not mean every low-dose approach is reckless. It means the phrase “microdosing” should not be treated as proven, gentle, or risk-free simply because it sounds smaller.
Does HRT Increase Breast Cancer Risk? What the Latest Evidence Says
Signs and Symptoms
a. Signs your symptoms may be perimenopause-related
Perimenopause can show up as:
- Hot flashes or night sweats
- Waking at 3 a.m. or struggling to stay asleep
- Irregular, heavier, lighter, shorter, or longer cycles
- New anxiety, irritability, low mood, or emotional sensitivity
- Brain fog or reduced concentration
- Weight gain around the middle
- Joint aches or muscle stiffness
- Vaginal dryness, bladder symptoms, or painful sex
- Lower libido
- New migraines or worsening premenstrual symptoms
NICE guidance covers the identification and management of menopause and aims to improve the consistency of support for people experiencing menopause symptoms. It was last reviewed in April 2026. (NICE)
b. Signs your symptoms may need metabolic assessment.
Before focusing on GLP-1 microdosing in perimenopause, it is worth checking whether there is a metabolic pattern that needs diagnosis and support.
Ask for a review if you notice:
- Rapid or unexplained weight gain
- Increased thirst or frequent urination
- Strong carbohydrate cravings with energy crashes
- Waist measurement is increasing despite no major lifestyle change
- High blood pressure
- Raised cholesterol or triglycerides
- Family history of type 2 diabetes or heart disease
- Previous gestational diabetes
- Fatty liver disease
- Symptoms of sleep apnoea, such as loud snoring or waking unrefreshed
c. Red flags that should not be dismissed
Seek medical advice promptly for:
- Bleeding after sex
- Bleeding after menopause
- Very heavy bleeding, flooding, or clots
- Sudden vision changes while using semaglutide
- Severe abdominal pain, especially with vomiting
- Chest pain, severe breathlessness, or one-sided leg swelling
- Severe depression, suicidal thoughts, or feeling unsafe
- Possible pregnancy while using a GLP-1 medicine
The UK MHRA advises that GLP-1 medicines should not be used during pregnancy or just before trying to conceive, and gives wash-out periods for semaglutide and tirzepatide before pregnancy attempts. It also highlights contraception considerations, especially with tirzepatide and oral contraceptives. (GOV.UK)
A note on medical advocacy
It is reasonable to say:
“I know weight can change in perimenopause, but this feels different for me. Can we check my metabolic health, thyroid function, menopause symptoms, medication history, and cardiovascular risk before deciding what support is appropriate?”
You do not need to apologise for wanting a proper explanation.
Diagnosis and Treatment
What assessment should come before GLP-1 treatment?
Before considering GLP-1 microdosing in perimenopause, a clinician may review:
- Weight history and waist measurement
- BMI, while acknowledging its limitations
- Blood pressure
- HbA1c or fasting glucose
- Lipid profile
- Liver function
- Kidney function
- Thyroid function
- Current medications
- Eating pattern and appetite changes
- Sleep, stress, alcohol intake, and activity level
- Menstrual pattern and menopause symptoms
- Pregnancy plans and contraception
- Personal or family history of pancreatitis, gallbladder disease, thyroid cancer, or severe gastrointestinal disease
This is not about gatekeeping. It is about avoiding the common midlife trap of treating a single symptom while overlooking the bigger picture.
Licensed GLP-1 treatment is not the same as microdosing
Licensed GLP-1 treatment follows approved indications, dose schedules, safety monitoring, and product standards. GLP-1 microdosing in perimenopause, especially through wellness clinics or compounded products, may not follow the same evidence base.
Semaglutide is prescription-only in the UK, and the NHS warns people using private prescriptions to buy from registered pharmacies because fake weight loss medicines are sold online. (nhs.uk)
Where HRT fits in
HRT, or hormone replacement therapy, replaces or supplements oestrogen and often progesterone to treat menopause symptoms. It is not a weight loss drug. But for suitable women, it may improve hot flashes, night sweats, sleep, mood symptoms, genitourinary symptoms, and quality of life.
This matters because some women pursue GLP-1 microdosing in perimenopause when their biggest driver is actually poor sleep from night sweats, anxiety, joint pain, or untreated vasomotor symptoms. If sleep improves, appetite regulation, energy, exercise tolerance, and cravings may also improve.
The British Menopause Society’s 2025 guidance specifically addresses incretin-based therapies in women using HRT, including considerations around co-prescribing during the menopause transition and postmenopause. (British Menopause Society)
What about oral hormones and contraceptives?
GLP-1 medicines can slow stomach emptying. This may matter for some oral medicines. The MHRA specifically notes that tirzepatide may reduce the effectiveness of oral contraceptives in people who are overweight or obese, advising additional barrier contraception for four weeks after starting and after dose increases, or switching to a non-oral method. (GOV.UK)
If you use oral progesterone, oral HRT, or the contraceptive pill, ask your clinician whether your medication route needs reviewing.
Barriers and Challenges
The wellness language can be misleading
The word “microdosing” sounds gentle. It suggests control, subtlety, and fewer side effects. But smaller does not automatically mean safer.
The risks depend on:
- The actual medicine
- The dose and frequency
- Whether it is licensed or compounded
- Your medical history
- Other medicines
- Hydration and nutrition status
- Pregnancy possibility
- Gallbladder and pancreas risk
- Monitoring and follow-up
A low dose of the wrong medicine, used for the wrong reason, without monitoring, can still cause harm.
Compounded and fake products are a real concern
WHO has warned that global demand for GLP-1 therapies has increased the spread of falsified and substandard products, creating patient safety risks. (World Health Organisation)
That matters because some “microdose” offers online may involve compounded products, unclear ingredients, non-standard units, or products purchased outside regulated prescribing channels.
Side effects may still happen
Common GLP-1 side effects can include:
- Nausea
- Vomiting
- Constipation
- Diarrhoea
- Reflux
- Reduced appetite
- Fatigue
- Headache
- Dizziness
- Dehydration if intake drops too low
More serious but less common concerns include gallbladder problems, pancreatitis, severe gastrointestinal symptoms, dehydration-related kidney strain, and rare eye complications reported with semaglutide. The MHRA advises urgent medical contact for sudden vision changes in people treated with semaglutide. (GOV.UK)
Midlife women are not a niche group
One major challenge is that midlife women are often treated as an afterthought in metabolic research. Yet perimenopause is a stage where cardiometabolic risk, sleep disruption, stress load, body composition, and hormone changes can overlap.
That is why GLP-1 microdosing in perimenopause needs better research, not louder marketing.
Solutions and Support
Clinical options to discuss
Depending on your symptoms and health profile, evidence-based support may include:
- Menopause assessment and discussion of HRT suitability
- Non-hormonal treatments for hot flashes if HRT is not suitable
- Screening for diabetes, thyroid disease, anaemia, lipid changes, and hypertension
- Referral to a specialist weight management service where appropriate
- Licensed GLP-1 treatment if you meet criteria
- Dietitian support
- Strength training guidance
- Sleep support
- Mental health support
- Review of medications that may contribute to weight gain
For some women, a GLP-1 medicine may be appropriate. For others, HRT, sleep treatment, resistance training, nutrition support, or thyroid care may be the missing piece.
Lifestyle care that is not “just lifestyle”
Lifestyle advice often sounds dismissive when it is thrown at women without assessment. But when done properly, it is powerful clinical care.
Helpful foundations include:
- Protein at meals to support muscle and appetite regulation
- Resistance training two to four times weekly to protect muscle and metabolic health
- Fibre-rich carbohydrates such as beans, lentils, oats, vegetables, berries, and whole grains
- Regular meal timing, if skipping meals, leads to evening overeating
- Sleep treatment, especially if night sweats, snoring, anxiety, or insomnia are present
- Alcohol review, because alcohol can worsen sleep, hot flashes, reflux, and weight gain
- Stress regulation, not as a cure-all, but because chronic stress can affect appetite, sleep, and energy
Questions to ask before trying GLP-1 microdosing
Before saying yes to GLP-1 microdosing in perimenopause, ask:
- What exact medicine is being prescribed?
- Is it licensed or compounded?
- What is the dose in milligrams, not vague “units”?
- What condition is being treated?
- Do I meet clinical criteria?
- What side effects should I watch for?
- What blood tests or follow-up will I need?
- Could this affect my contraception, HRT, or other medicines?
- What happens if I stop?
- How will we protect muscle, nutrition, and bone health?
- What is the plan if I cannot get enough protein or if I become constipated, dizzy, or fatigued?
A balanced way to think about it
GLP-1 microdosing in perimenopause should not be framed as either a miracle or a menace. The more accurate view is this:
GLP-1 medicines are legitimate medical treatments for specific indications. Perimenopausal metabolic changes are real. Some women may benefit from GLP-1 therapy under appropriate medical supervision. But the microdosing trend is ahead of the evidence, especially when sold as a low-risk wellness hack.
Conclusion
Perimenopause can make a woman feel like she is living in a body with new rules and no instruction manual. So when GLP-1 microdosing in perimenopause is presented as a gentler, smarter, more tailored option, the appeal is obvious.
But “gentle” should mean carefully assessed, medically supervised, evidence-informed, and safe — not vague, unregulated, or driven by influencer language.
The best starting point is not shame. It is information. If your weight, cravings, blood sugar, sleep, or appetite have changed in midlife, you deserve a proper assessment. You deserve to be listened to. And you deserve care that looks at the whole picture: hormones, metabolism, sleep, stress, muscle, nutrition, medication safety, and your actual life.
Takeaway
Summary box: What to do next
- Do not start GLP-1 microdosing in perimenopause without medical supervision.
- Ask for a metabolic health review if weight gain, cravings, fatigue, or blood sugar symptoms feel new or worsening.
- Review menopause symptoms separately; untreated night sweats, insomnia, and anxiety can worsen appetite and weight patterns.
- Be cautious with compounded, fake, or online GLP-1 products.
- Ask about contraception and pregnancy planning before using GLP-1 medicines.
- Protect muscle with protein, resistance training, and adequate nutrition.
- Seek urgent help for severe abdominal pain, sudden vision changes, pregnancy, chest pain, severe dehydration, or concerning mental health symptoms.
Not sure where your symptoms fit? Take the Tools and Quizzes to understand your pattern.
Frequently Asked Questions
1. Is GLP-1 microdosing in perimenopause safe?
There is not enough long-term evidence to say that GLP-1 microdosing in perimenopause is safe or effective as a general wellness strategy. GLP-1 medicines should only be used when prescribed by a qualified clinician, with a clear reason, proper dosing, and monitoring.
2. Can GLP-1 medicines help with menopause weight gain?
They may help some women with obesity, type 2 diabetes, or weight-related metabolic risk. But menopause-related weight change can have several causes, including sleep disruption, muscle loss, insulin resistance, thyroid disease, stress, medication effects, and untreated menopause symptoms.
3. Is microdosing the same as starting on a low dose?
Not necessarily. Many licensed GLP-1 medicines already start at a lower dose and increase gradually to reduce side effects. That is not the same as unregulated “microdosing” or the use of non-standard compounded products.
4. Can I take GLP-1 medicines with HRT?
Some women may use GLP-1 medicines and HRT together under medical supervision. However, the British Menopause Society has highlighted specific considerations for women using incretin-based therapies alongside HRT, so this should be reviewed with a clinician. (British Menopause Society)
5. Can GLP-1 medicines affect contraception?
Yes, this can matter. The MHRA advises additional precautions with tirzepatide and oral contraceptives after starting treatment and after dose increases, because effectiveness may be reduced in some people. (GOV.UK)
6. Will GLP-1 microdosing balance my hormones?
There is no good evidence that GLP-1 microdosing in perimenopause “balances hormones.” GLP-1 medicines act mainly on appetite, blood sugar, insulin response, digestion, and weight-related pathways. Menopause symptoms need their own assessment.
7. What should I try before GLP-1 microdosing?
Start with a proper clinical review. Ask about menopause care, blood sugar, thyroid function, cholesterol, blood pressure, sleep, medications, nutrition, and strength training. If GLP-1 treatment is appropriate, it should be prescribed safely and monitored.
Medical Disclaimer
This article is for educational purposes only and does not replace personalised medical advice, diagnosis, or treatment. If you are worried about your symptoms, if your symptoms are getting worse, or if something does not feel right in your body, please speak with your doctor, nurse practitioner, gynaecologist, endocrinologist, or another qualified healthcare professional. Seek urgent medical help for severe, sudden, or concerning symptoms.