Introduction:
If you have been thinking about HRT but feel nervous because of breast cancer headlines, you are not alone. HRT and breast cancer risk is one of the most searched, most misunderstood, and most emotionally loaded menopause topics. Many women are left wondering: Am I putting myself in danger, or am I avoiding treatment that could genuinely help me feel well again?
The clearest answer is this: HRT and breast cancer risk depend on the type of HRT, how long it is used, your personal breast cancer risk, and whether you have a uterus or a history of breast cancer. NICE says oestrogen-only HRT has little or no increase in breast cancer risk, while combined HRT can increase risk, especially with longer use. (NICE)
In this article, we will walk through what the evidence actually means, what is worth paying attention to, and how to have a calm, informed conversation with your clinician.
What Is Hormone Replacement Therapy?
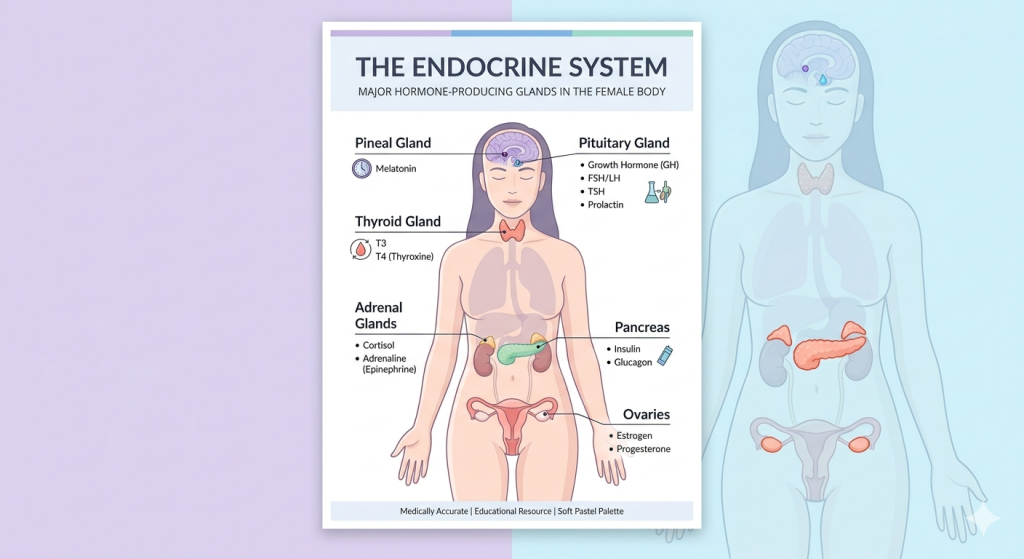
HRT, or hormone replacement therapy, is treatment used to replace or support falling hormone levels during perimenopause and menopause. It is most often used to help symptoms such as hot flushes, night sweats, poor sleep, vaginal dryness, low mood, joint aches, brain fog, and reduced quality of life.
There are different types:
- Oestrogen-only HRT: usually for women who have had a hysterectomy.
- Combined HRT: oestrogen plus a progestogen, used when the uterus is still present to protect the womb lining.
- Vaginal oestrogen: low-dose local treatment for vaginal dryness, bladder symptoms, painful sex, and recurrent urinary symptoms.
- Systemic HRT: tablets, patches, gels, sprays, or implants that affect the whole body.
When people talk about HRT and breast cancer risk, they are usually talking about systemic HRT, especially combined oestrogen-progestogen therapy. Low-dose vaginal oestrogen is generally treated differently because very little is absorbed into the bloodstream, and major guidance does not link it with the same breast cancer risk pattern as systemic therapy. (The Lancet)
FemPhases Menopause Symptom Checker
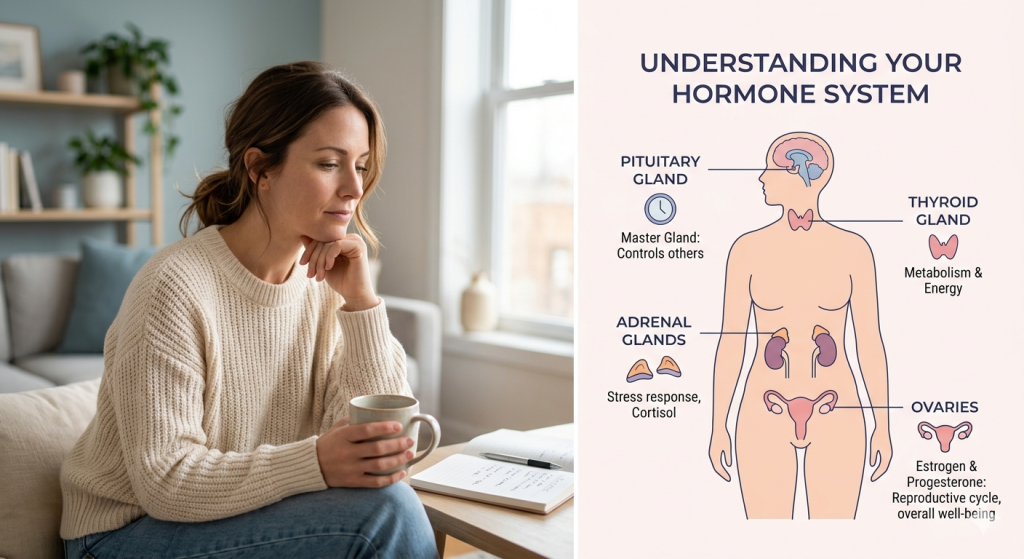
Why Does It Happen?
Breast tissue is hormone-sensitive. Oestrogen and progesterone can influence the growth of some breast cells. This does not mean HRT “automatically causes cancer,” but it helps explain why certain hormone combinations may slightly increase the chance of breast cancer being diagnosed in some women.
i. The type of HRT matters
The latest guidance consistently separates oestrogen-only HRT from combined HRT. NICE states there is “very little or no increase” in breast cancer risk with oestrogen-only HRT, while combined HRT is associated with an increased risk. (NICE)
Combined HRT is often necessary for women with a uterus because taking oestrogen without enough progestogen can increase the risk of endometrial cancer. So this is not about one hormone being “good” and another being “bad.” It is about matching the safest treatment to your body.
ii. Duration matters
The longer systemic HRT is used, the more important individual risk review becomes. The large 2019 Lancet individual participant meta-analysis found that breast cancer risk increased with duration of menopausal hormone therapy use, except for vaginal oestrogens. (The Lancet)
That does not mean every woman must stop HRT after a set number of years. It means the decision should be reviewed regularly, especially if symptoms or risk factors have changed, or the original reason for starting HRT has changed.
iii. Your baseline risk matters
A small relative increase can mean different things for different women. A woman with a strong family history, previous high-risk breast biopsy, dense breasts, obesity, high alcohol intake, or previous breast cancer may need more specialist guidance than someone with low baseline risk.
The British Menopause Society highlights that HRT risk should be discussed alongside other breast cancer risk factors, including alcohol and obesity, rather than in isolation. (British Menopause Society)
Signs and Symptoms
HRT and breast cancer risk is not usually something you can “feel.” Breast cancer risk is about probability, not a pattern of symptoms. Still, breast awareness matters whether you use HRT or not.
Common menopause symptoms that may lead women to consider HRT include:
- Hot flushes
- Night sweats
- Waking at 3–4 a.m.
- Mood changes or anxiety
- Brain fog
- Vaginal dryness or soreness
- Painful sex
- Recurrent urinary symptoms
- Joint aches
- Palpitations
- Low libido
- Fatigue
- Skin and hair changes
Breast changes that should be checked include:
- A new breast lump or thickening
- Nipple discharge, especially if bloody
- New nipple inversion
- Dimpling or puckering of breast skin
- A rash or crusting around the nipple
- Persistent breast pain in one area
- Swelling, redness, or warmth
- A lump in the armpit
- Any change that feels unusual for you

What Is Normal and When to Pay Attention?
Some breast tenderness can happen when starting or adjusting HRT, especially if the dose or progestogen pattern changes. But new, persistent, one-sided, or unusual breast changes should always be assessed.
a. Common Changes
These may be common but are still worth monitoring:
- Mild breast tenderness after starting HRT
- Temporary bloating or fluid retention
- Light bleeding in the first few months of some HRT regimens
- Changes in sleep, mood, or energy while adjusting treatment
- Vaginal discharge with local oestrogen
- Cyclical breast discomfort with sequential combined HRT
b. Needs Urgent Attention
Do not ignore:
- A new breast lump
- Nipple bleeding or new discharge
- Bleeding after sex
- Heavy or persistent abnormal bleeding
- Severe pelvic pain
- Chest pain, shortness of breath, fainting, or sudden weakness
- Symptoms of anaemia, such as breathlessness, dizziness, or extreme fatigue
- Unexplained weight loss
- Severe mood changes or thoughts of self-harm
Evidence-Based Solutions
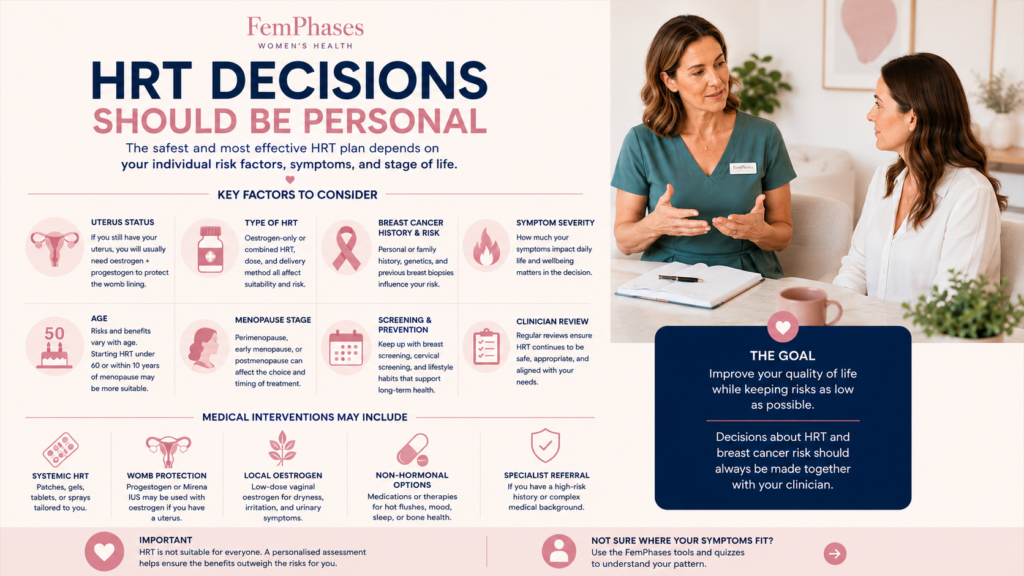
The safest approach to HRT and breast cancer risk is not panic or avoidance. It is personalised decision-making.
A good menopause consultation should consider:
- Your age
- Menopause stage
- Whether you have a uterus
- Personal or family history of breast cancer
- Previous breast biopsies or genetic risk
- Your symptoms and how much they affect daily life
- Blood clot, stroke, heart disease, and migraine history
- Bone health
- Current medicines
- Your values and preferences
For many healthy women under 60, or within 10 years of menopause, HRT can be an appropriate and effective treatment for menopause symptoms when benefits outweigh risks. NICE recommends providing women with clear information about benefits and risks so that decisions can be individualised. (NICE)
Bleeding After 40: When Irregular Bleeding Needs a Medical Check
Medical Interventions
Medical assessment
Before starting HRT, your clinician may ask about:
- Menstrual pattern
- Last period
- Pregnancy possibility, if relevant
- Breast symptoms
- Family history of breast, ovarian, womb, or bowel cancer
- Blood pressure
- Weight and cardiovascular risk
- Migraine, clotting history, liver disease, or unexplained bleeding
Routine hormone blood tests are not always needed to diagnose menopause in women over 45 with typical symptoms. Still, tests may be useful in younger women, complex cases, early menopause, or when another condition may be involved.
Choosing the type of HRT
For women with a uterus, combined HRT is usually needed to protect the womb lining. For women without a uterus, oestrogen-only HRT may be suitable and appears to carry little or no increase in breast cancer risk according to NICE. (NICE)
Options may include:
- Oestrogen patch, gel, spray, or tablet
- Micronised progesterone
- Combined patches or tablets
- Mirena intrauterine system for womb protection in some women
- Low-dose vaginal oestrogen for genitourinary symptoms
- Non-hormonal medicines for hot flushes if HRT is unsuitable
If you have had breast cancer
This needs specialist advice. Systemic HRT is often avoided after breast cancer, especially hormone receptor-positive breast cancer, but decisions can be complex and should involve oncology or breast specialists. BMS guidance notes that low-dose vaginal oestrogen may be considered in some situations after discussion with the breast care team. However, extra caution is needed for women taking aromatase inhibitors. (British Menopause Society)
Holistic and Lifestyle Support
Lifestyle support cannot “cancel out” HRT and breast cancer risk, but it can improve menopause symptoms and support long-term health.
Helpful foundations include:
- Protein at each meal: supports muscle, metabolism, and blood sugar stability.
- Fibre-rich foods: vegetables, beans, lentils, oats, berries, nuts, and seeds support gut and heart health.
- Blood sugar balance: regular meals with protein, fibre, and healthy fats may reduce energy crashes and mood swings.
- Strength training: helps protect bones and muscles, improves insulin sensitivity, and boosts confidence.
- Alcohol reduction: alcohol is a recognised breast cancer risk factor, so reducing intake is a meaningful step.
- Sleep support: regular wake times, morning light, and reducing late caffeine can help.
- Stress management: breathing exercises, therapy, journaling, and boundaries can calm the nervous system.
- Symptom tracking: track hot flushes, sleep, bleeding, breast symptoms, mood, and medication changes.
- Supplement safety: avoid using supplements as hormone “cures.” Check interactions, especially if you take cancer medication, blood thinners, antidepressants, or thyroid medicine.
When to See a Doctor
Book a review if menopause symptoms are affecting your sleep, work, relationships, mood, sex life, or daily functioning. You deserve proper support, not dismissal.
Seek medical advice promptly for:
- New breast changes
- Heavy bleeding
- Bleeding after sex
- Bleeding after menopause
- Severe pelvic pain
- Unexplained weight loss
- Symptoms of anaemia
- Pregnancy concerns
- Severe mood changes
Seek urgent help for chest pain, shortness of breath, fainting, sudden weakness, or thoughts of self-harm.
Key Takeaway
HRT and breast cancer risk is real but often misunderstood. The risk depends mainly on the type of HRT, duration of use, and your personal baseline risk. Oestrogen-only HRT has little or no increase in breast cancer risk in NICE guidance, while combined HRT can increase risk, especially with longer use. (NICE)
Track your symptoms, stay breast aware, keep up with screening, and speak with a clinician who can help you weigh benefits and risks in the context of your actual life.
Frequently Asked Questions
1: Does HRT cause breast cancer?
HRT may increase the risk of breast cancer being diagnosed, especially combined HRT used for longer periods. The level of risk depends on the type of HRT and personal risk factors.
2: Is oestrogen-only HRT safer for breast cancer risk?
For women who can use it, oestrogen-only HRT is associated with little or no increase in breast cancer risk according to NICE. (NICE)
3: Is combined HRT dangerous?
Not automatically. Combined HRT can increase breast cancer risk, but it may still be appropriate when symptoms are significant, and benefits outweigh risks. It also protects the womb lining in women with a uterus.
4: Does vaginal oestrogen increase breast cancer risk?
Low-dose vaginal oestrogen is not treated the same as systemic HRT and is generally considered to have minimal systemic absorption. It should still be discussed with a clinician, especially after breast cancer.
5: Can I take HRT if breast cancer runs in my family?
Possibly, but you need an individual risk assessment. Family history, genetics, breast screening history, and symptom severity all matter.
6: How often should HRT be reviewed?
Usually at least yearly, or sooner if symptoms change, side effects occur, bleeding develops, or your breast cancer risk profile changes.
7: What can I do instead of HRT?
Options include lifestyle changes, CBT for symptom coping, vaginal moisturisers, non-hormonal medicines for flushes, sleep support, and targeted treatment for mood, bladder, or sexual symptoms.
Not sure where your symptoms fit? Take the Tools and Quizzes to understand your pattern.
Medical Disclaimer
This article is for educational purposes only and does not replace personalised medical advice, diagnosis, or treatment. If you are worried about your symptoms, if your symptoms are getting worse, or if something does not feel right in your body, please speak with your doctor, nurse practitioner, gynaecologist, endocrinologist, or another qualified healthcare professional. Seek urgent medical help for severe, sudden, or concerning symptoms.