Introduction
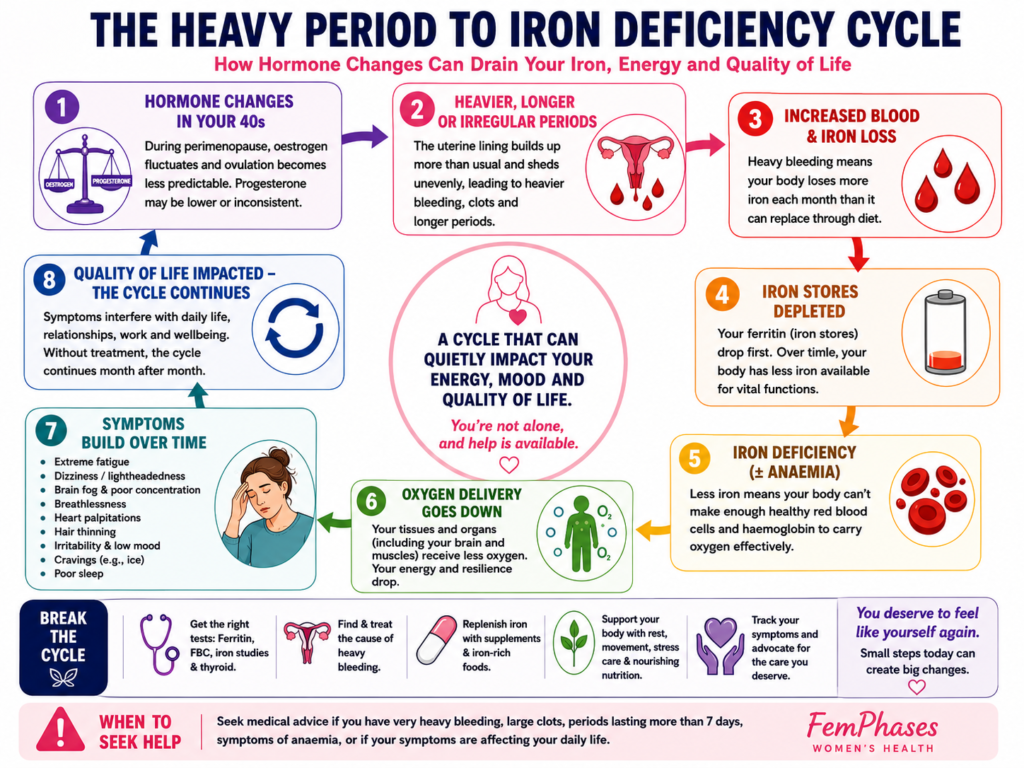
For many women, the 40s arrive with subtle shifts at first: a missed period here, a shorter cycle there, a little more fatigue than usual. Then sometimes the changes become impossible to ignore. Periods get heavier. Clots appear. Bleeding lasts longer. Energy disappears.
You may find yourself wondering whether this is “just perimenopause” or whether something more serious is happening.
Heavy periods and low iron in your 40s are common, but understanding that you don’t have to endure them can empower you to seek evaluation, especially during the menopausal transition, also called perimenopause, the hormonal phase leading up to menopause. Remember, common does not mean normal.
Heavy menstrual bleeding can quietly drain iron stores over months or years, leading to iron deficiency and, in some cases, iron-deficiency anaemia a condition where the body no longer has enough healthy red blood cells to carry oxygen effectively.
The effects can be profound:
- Exhaustion that sleep does not fix
- Brain fog and poor concentration
- Breathlessness
- Anxiety-like symptoms
- Heart palpitations
- Hair shedding
- Feeling physically “flattened”
Recent guidance from organisations including the National Institute for Health and Care Excellence, the American College of Obstetricians and Gynaecologists, and the World Health Organisation continues to emphasise that heavy bleeding warrants proper evaluation, particularly during midlife, when hormonal fluctuations can overlap with fibroids, thyroid conditions, adenomyosis, and other health concerns.
Understanding the connection between hormones, bleeding, and iron levels can help you advocate for yourself earlier. Keeping track of your symptoms can build confidence in discussing your health and making informed decisions.
Am I in Perimenopause? Symptom Quiz
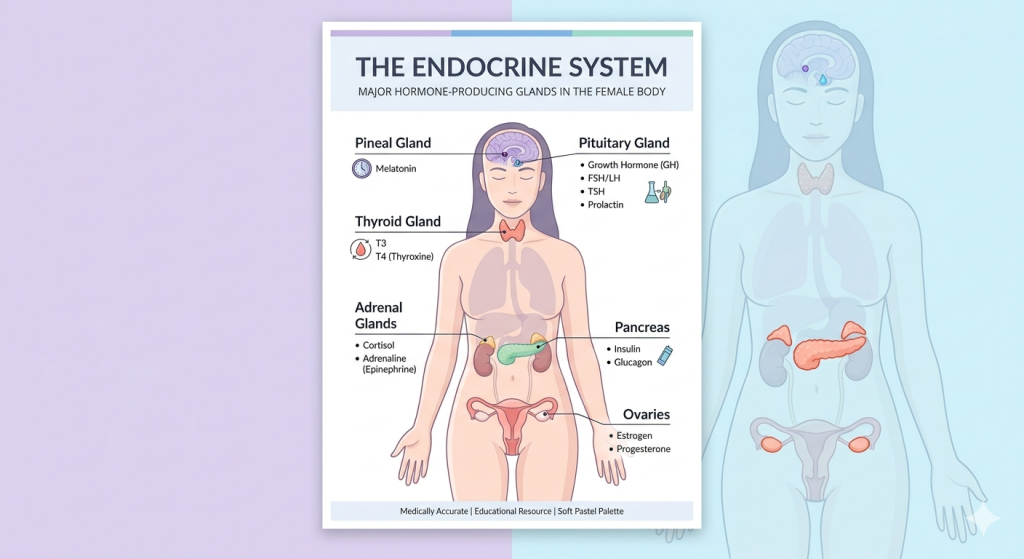
Why Heavy Bleeding Often Increases During Perimenopause
Fluctuating levels of oestrogen and progesterone mark perimenopause. These hormones help regulate the menstrual cycle and maintain the lining of the uterus (the endometrium).
During your 40s, ovulation becomes less predictable. Many cycles become anovulatory, meaning the ovary does not release an egg. Without ovulation, progesterone levels may remain lower than usual while oestrogen continues stimulating the uterine lining.
The result?
The lining can build up excessively and shed irregularly, causing:
- Heavier bleeding
- Longer periods
- Shorter cycles
- Spotting between periods
- Large blood clots
Research published across 2024–2026 women’s health reviews continues to show that hormonal instability during perimenopause is one of the leading causes of abnormal uterine bleeding in midlife women.
i. The Iron Loss Connection
Iron is essential for producing haemoglobin, the protein in red blood cells that carries oxygen throughout the body.
When menstrual bleeding becomes excessive, the body can lose iron faster than it replaces it.
Over time, this may progress through stages:
- Iron depletion: stored iron falls
- Iron deficiency: tissues begin to lack iron
- Iron-deficiency anaemia: haemoglobin drops
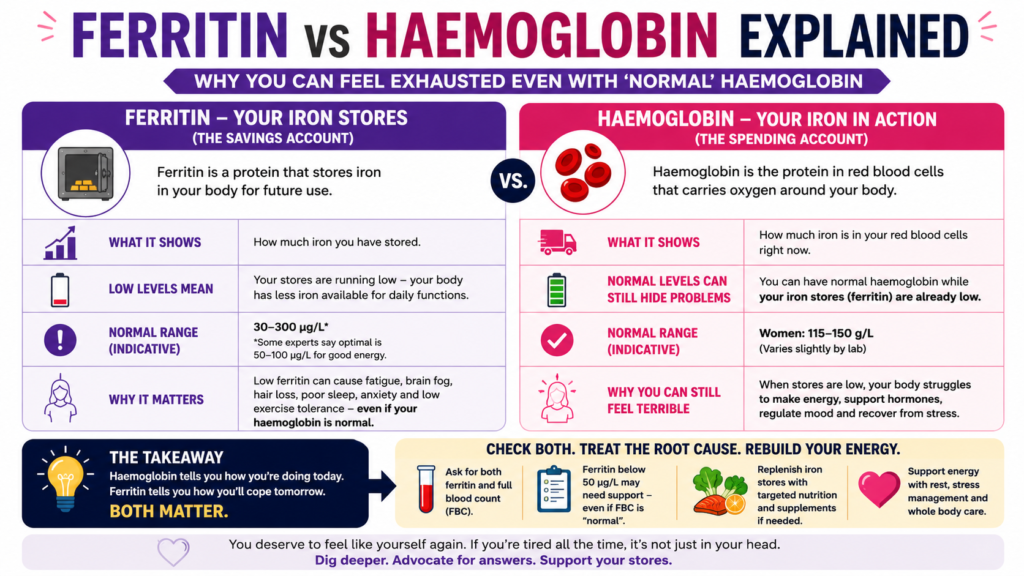
Importantly, many women experience symptoms even before anaemia appears on standard blood tests.
This is why some clinicians now recommend evaluating:
- Ferritin (iron storage protein)
- Full blood count (FBC)
- Transferrin saturation
- Vitamin B12 and folate
- Thyroid function
A “normal” haemoglobin result does not always rule out iron deficiency.
ii. Fibroids, Adenomyosis, and Other Hidden Causes
Not all heavy bleeding in your 40s is purely hormonal. Conditions such as fibroids, adenomyosis, thyroid disorders, endometrial polyps, and endometriosis can also contribute to heavy periods and should be considered during evaluation.
Several conditions become more common during this stage of life.
Fibroids are non-cancerous growths in or around the uterus that can increase bleeding, pressure, pelvic pain, and urinary symptoms.
Adenomyosis occurs when tissue similar to the uterine lining grows into the muscular wall of the uterus. It can cause:
- Very painful periods
- Heavy clotting
- Pelvic pressure
- Chronic inflammation
Other possible contributors include:
- Thyroid disorders
- Endometrial polyps
- Endometriosis
- Bleeding disorders
- Certain medications
- Perimenopausal hormonal changes
- Rarely, endometrial cancer
This is why persistent heavy bleeding should never automatically be dismissed as “just age.”
iii. Why Iron Deficiency Affects the Whole Body
Iron is involved in far more than oxygen transport.
Low iron can affect:
- Brain function
- Neurotransmitters
- Temperature regulation
- Muscle performance
- Immune function
- Hair growth
- Mood regulation
Emerging evidence also suggests links between iron deficiency and:
- Increased anxiety symptoms
- Restless legs syndrome
- Sleep disruption
- Reduced exercise tolerance
Many women describe it as feeling unlike themselves.
Symptoms, Diagnosis & Barriers
1. Signs Your Heavy Periods May Be Affecting Iron Levels
Symptoms can develop gradually and become easy to normalise.
Common signs include:
- Extreme fatigue
- Needing naps frequently
- Breathlessness climbing stairs
- Dizziness
- Pale skin
- Heart palpitations
- Headaches
- Hair thinning
- Feeling cold often
- Poor concentration or “brain fog”
- Irritability
- Weakness
- Craving ice or non-food items (pica)
Signs of heavy menstrual bleeding itself may include:
- Bleeding through pads or tampons hourly
- Passing clots larger than a 50p coin
- Bleeding longer than 7 days
- Needing double protection
- Waking overnight to change products
- Avoiding social activities due to bleeding
ii. When Heavy Bleeding Needs Urgent Medical Assessment
When heavy bleeding becomes severe or sudden, seek prompt medical assessment. Urgent signs include passing large clots, fainting, chest pain, or bleeding after menopause, which require immediate attention. Seek prompt medical care if you experience:
- Sudden severe bleeding
- Fainting or chest pain
- Shortness of breath
- Bleeding after sex
- Bleeding after menopause
- Severe pelvic pain
- Rapid worsening of symptoms
iii. The Problem of Medical Dismissal
Many women spend years being told:
- “Your labs are normal.”
- “It’s just stress.”
- “It’s your age.”
- “Perimenopause is messy.”
While hormonal shifts are real, your persistent symptoms deserve investigation. You have the right to be heard and taken seriously when discussing your health concerns.
Women in midlife are often balancing careers, caregiving, mental load, and chronic exhaustion. Symptoms become easy to minimise — both internally and within healthcare systems.
Medical advocacy matters.
It is reasonable to ask:
- What is causing my bleeding?
- Has my ferritin been checked?
- Could this be fibroids or adenomyosis?
- Should I have imaging or further testing?
- What are my treatment options?
iv. Recommended Diagnostic Approaches
Depending on symptoms and history, evaluation may include:
- Pelvic examination
- Blood tests
- Pelvic ultrasound
- Endometrial biopsy
- Hysteroscopy
- Hormone evaluation
- Thyroid testing
Current guidelines from NICE and ACOG support investigating abnormal bleeding patterns during perimenopause, particularly when bleeding changes significantly or impacts quality of life.
Waking Up at 3AM in Perimenopause
Solutions & Support
i. Iron Replacement and Nutritional Support
If iron deficiency is confirmed, treatment may involve oral iron supplements or, in more severe cases, intravenous iron infusions.
Many women struggle with gastrointestinal side effects from iron tablets, including constipation and nausea. Newer evidence suggests that:
- Lower-dose iron
- Alternate-day dosing
- Taking iron with vitamin C
- may improve absorption and tolerability.
Iron-rich foods include:
- Lean red meat
- Lentils
- Beans
- Spinach
- Pumpkin seeds
- Sardines
- Tofu
Pairing plant-based iron with vitamin C sources can improve absorption.
ii. Hormonal Treatments for Heavy Bleeding
Treatment depends on the underlying cause, symptom severity, age, fertility goals, and overall health.
Evidence-based options may include:
- Levonorgestrel intrauterine system (LNG-IUS) — a hormone-releasing coil that can significantly reduce bleeding
- Combined hormonal contraception
- Cyclical progesterone therapy
- Hormone replacement therapy adjustments
- Tranexamic acid (a medication that reduces bleeding)
- Non-steroidal anti-inflammatory drugs (NSAIDs)
For some women, addressing hormonal imbalance improves both bleeding and iron levels dramatically.
iii. Surgical and Procedural Options
When symptoms are severe or structural conditions are present, procedures may be recommended.
These can include:
- Fibroid removal (myomectomy)
- Endometrial ablation
- Uterine artery embolisation
- Hysterectomy
Treatment decisions should always involve informed discussion about benefits, risks, recovery, and long-term effects.
iv. Lifestyle and Nervous System Support
Heavy bleeding and chronic iron depletion affect more than physical health. They can deeply impact emotional well-being, identity, confidence, relationships, and work life.
Supportive strategies may include:
- Gentle movement during recovery
- Sleep optimisation
- Anti-inflammatory nutrition
- Stress reduction
- Trauma-informed care
- Pelvic floor physiotherapy
- Mental health support
You do not need to “earn” rest by collapsing first.
v. The Importance of Tracking Symptoms
Tracking cycles can reveal patterns that are difficult to remember during appointments.
Consider recording:
- Bleeding days
- Clotting
- Fatigue severity
- Mood changes
- Pain
- Dizziness
- Sleep changes
This information can strengthen medical conversations and improve diagnostic accuracy.
Conclusion
Heavy periods during your 40s are common, but they are not something you have to tolerate in silence.
When bleeding becomes excessive, the body can quietly slide into iron depletion and exhaustion that affects nearly every system — physical, emotional, and cognitive.
The good news is that there are real explanations, real investigations, and real treatments available.
The Femphases Takeaway
If your periods have become heavier, longer, or more draining in your 40s:
- Do not assume it is “just ageing”
- Ask for iron studies, including ferritin
- Track symptoms and bleeding patterns
- Seek evaluation for fibroids, adenomyosis, and hormonal changes
- Know that exhaustion is not a personality trait
- Advocate for yourself if symptoms are dismissed
- Remember that treatment should support your quality of life, not just survival
Your body is communicating something important. You deserve to listen to it and to be listened to in return.
Frequently Asked Questions
1. Can perimenopause cause very heavy periods?
Yes. Hormonal fluctuations during perimenopause can cause the uterine lining to build up unevenly, leading to heavier or more prolonged bleeding.
2. What ferritin level is considered low in women?
Ranges vary by laboratory, but many experts recognise that women may experience symptoms even when ferritin falls within “low-normal” ranges.
3. Can low iron cause anxiety symptoms?
Yes. Iron deficiency may contribute to fatigue, palpitations, poor concentration, irritability, and anxiety-like symptoms.
4. Are blood clots during periods normal in your 40s?
Small clots can occur occasionally, but large or frequent clots may indicate heavy menstrual bleeding and should be assessed.
5. When should heavy bleeding be investigated?
If bleeding changes suddenly, lasts longer than 7 days, causes severe fatigue, includes large clots, or affects daily life, medical assessment is recommended.
6. Can fibroids worsen during perimenopause?
Yes. Fibroids may continue causing symptoms during perimenopause, particularly if oestrogen levels fluctuate significantly.
7. Is iron deficiency common in women over 40?
Very common. Heavy menstrual bleeding remains one of the leading causes of iron deficiency in midlife women.
Soft Call to Action
Not sure where your symptoms fit? Take the Tools and Quizzes to understand your pattern.
Medical Disclaimer
This article is for educational purposes only and does not replace personalised medical advice, diagnosis, or treatment. If you are worried about your symptoms, if your symptoms are getting worse, or if something does not feel right in your body, please speak with your doctor, nurse practitioner, gynaecologist, endocrinologist, or another qualified healthcare professional. Seek urgent medical help for severe, sudden, or concerning symptoms.