
Introduction
Bone health is one of those things many women only think about after a scan, a fracture, or a quiet comment from a doctor: “Your bone density is lower than expected.” But your bones are not fixed structures. They are living tissue, constantly breaking down and rebuilding. That is why Vitamin D3 and K2 for bone health matter so much, especially during perimenopause, menopause, postmenopause, pregnancy, breastfeeding, and later life.
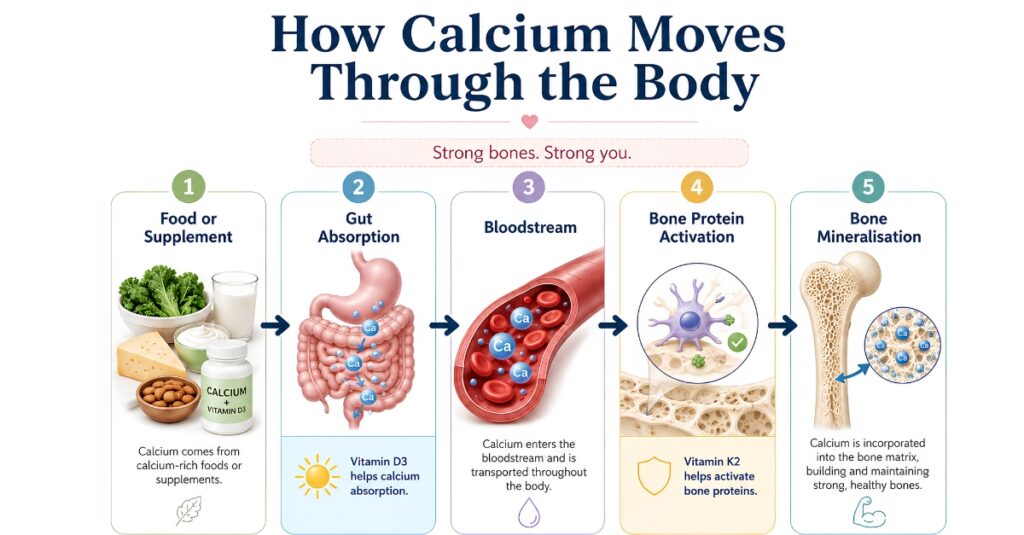
Vitamin D3 helps your body absorb and regulate calcium. Vitamin K2 helps activate proteins that direct calcium into bone tissue. Think of D3 as helping calcium get through the door, and K2 as helping guide it to the right room. That does not mean everyone needs high-dose supplements, and it certainly does not mean supplements cure osteoporosis. But it does mean that Vitamin D3 and K2 for bone health deserve a thoughtful, evidence-based conversation.
The Overview
Bone health becomes especially important for women because oestrogen supports bone remodelling, the normal cycle in which old bone is broken down and new bone is formed. As oestrogen levels fluctuate and decline during perimenopause and menopause, bone loss can speed up. This is one reason osteoporosis is more common after menopause.
Osteoporosis means bones have become more fragile, increasing the chance of fractures, especially in the hip, spine, and wrist. Osteopenia means bone density is lower than expected but not low enough to be diagnosed as osteoporosis.
Vitamin D has a well-established role in bone health because it helps regulate calcium and phosphate. NHS guidance states that these nutrients are needed to keep bones, teeth, and muscles healthy. (nhs.uk) Vitamin K2 is less widely discussed in standard public guidance. Still, growing research suggests it may support bone metabolism by activating vitamin K-dependent proteins such as osteocalcin, which binds calcium in bone. (MDPI)
So when people talk about Vitamin D3 and K2 for bone health, the real message is this: bones need nutrients, hormones, movement, and medical risk assessment working together.
The In-Depth Study
How Vitamin D3 Supports Bone Strength
Vitamin D3, also called cholecalciferol, is one of the main forms of vitamin D used in supplements. It helps the gut absorb calcium from food and supplements. Without enough vitamin D, your body may struggle to maintain healthy calcium levels, and over time, this can weaken bones.
The NIH explains that 25-hydroxyvitamin D, often written as 25(OH)D, is the main blood test used to assess vitamin D status. The NIH also notes that levels of 50 nmol/L (20 ng/mL) are considered sufficient for most people, while the risk of deficiency rises below 30 nmol/L (12 ng/mL). (Office of Dietary Supplements)
This matters because many women are told to “just take calcium,” but calcium alone is not the whole story. Your body needs enough vitamin D to absorb and use calcium effectively.
How Vitamin K2 Helps Calcium Go Where It Is Needed
Vitamin K2 belongs to the vitamin K family. It is found in forms called menaquinones, including MK-4 and MK-7. Vitamin K2 helps activate proteins such as osteocalcin, a protein made by bone-building cells called osteoblasts. Activated osteocalcin helps bind calcium into the bone matrix.
A 2024 review in Nutrients describes vitamin K as necessary for the carboxylation of osteocalcin and matrix Gla protein, both of which are involved in calcium handling and bone mineralisation. (MDPI) A 2024 systematic review and meta-analysis also found that vitamin K, especially K2, may help maintain or increase lumbar spine bone mineral density. However, the quality of the evidence and the populations studied vary. (PMC)
That is why Vitamin D3 and K2 for bone health are often described as a “power couple”: D3 supports calcium absorption, while K2 supports calcium-related bone proteins.
Why This Does Not Mean “More Is Better”
More is not always better with supplements. Vitamin D is fat-soluble, which means excess amounts can build up. The NIH warns that vitamin D toxicity can cause high calcium levels, kidney problems, soft tissue calcification, abnormal heart rhythms, and other serious effects, usually from excessive supplement intake. (Office of Dietary Supplements)
The Endocrine Society’s 2024 guideline also takes a cautious approach. It states that most healthy adults under 75 are unlikely to benefit from taking more than the recommended daily allowance of vitamin D, and that routine vitamin D testing is not needed for most healthy people. (Endocrine)
So yes, Vitamin D3 and K2 for bone health can be important. But safe, personalised use matters.
Menopause, Oestrogen, and Bone Loss
During menopause, declining oestrogen can increase bone turnover. This means bone may be broken down faster than it is rebuilt. This is why conversations about bone health often become more urgent in the 40s, 50s, and beyond.
The British Menopause Society states that adequate dietary or supplemental calcium and vitamin D are part of osteoporosis management, while also making clear that calcium and vitamin D alone have mixed evidence for reducing fractures and should not be seen as the only treatment. (British Menopause Society)
For some women, medical treatments such as hormone replacement therapy, bisphosphonates, denosumab, or other osteoporosis medicines may be appropriate. Nutrients are foundational, but they are not a substitute for clinically indicated treatment.
Signs and Symptoms
Low vitamin D, low calcium intake, and declining bone density can be silent for years. Many women feel completely well until they have a fracture or a bone density scan.
a. Possible Signs of Low Vitamin D
Some people with low vitamin D may notice:
- Bone aches or tenderness
- Muscle weakness
- Fatigue
- Increased falls or poor muscle function
- Low mood, although this is non-specific
- Slow recovery from aches and pains
These symptoms can also come from many other causes, including thyroid problems, anaemia, menopause-related sleep disruption, inflammatory conditions, medication side effects, or stress. That is why symptoms should be assessed rather than guessed.
b. Possible Signs of Bone Loss
Osteopenia and osteoporosis often do not cause symptoms early on. Warning signs may include:
- A fracture from a minor fall
- Loss of height over time
- New spinal curvature
- Sudden back pain after lifting, coughing, or bending
- Family history of hip fracture or osteoporosis
- Long-term steroid use
- Early menopause or surgical menopause
c. When to Advocate for Medical Review
Ask your doctor, nurse practitioner, gynaecologist, endocrinologist, or menopause clinician about bone health if you have:
- Menopause before age 45
- History of eating disorders or very low body weight
- Coeliac disease, inflammatory bowel disease, or malabsorption
- Long-term steroid medication use
- Previous low-trauma fracture
- Strong family history of osteoporosis
- Long gaps without periods before menopause
- Breast cancer treatment or medicines that lower oestrogen
- Recurrent falls
This is where Vitamin D3 and K2 for bone health should become part of a wider discussion, not a quick supplement purchase.
Diagnosis and Treatment
i. Blood Tests
A vitamin D blood test usually measures 25-hydroxyvitamin D, the main marker of vitamin D status. Testing may be useful if there are symptoms, risk factors, bone disease, malabsorption, kidney disease, certain medications, or a clinician suspects deficiency.
A 2025 NHS formulary guidance document categorises serum 25(OH)D below 25 nmol/L as deficiency, 25–50 nmol/L as insufficiency, and above 50 nmol/L as normal range. (Shropshire and Telford Formulary) Local thresholds may vary, so a qualified clinician should interpret results.
ii. Bone Density Scan
A DEXA scan, also called a DXA scan, measures bone mineral density. It can help diagnose osteopenia or osteoporosis and guide treatment decisions. Your clinician may also use fracture-risk tools to estimate your future fracture risk.
iii. Supplement Dosing Should Be Personalised
Vitamin D dosing depends on age, diet, sunlight exposure, skin tone, pregnancy status, medical conditions, medications, and blood results. NHS public guidance advises that people in the UK consider taking a daily vitamin D supplement during autumn and winter, and that some people at higher risk may need it year-round. (nhs.uk)
Vitamin K2 dosing is less standardised in mainstream guidelines. It may be considered in some people, but it should be used carefully, especially if you take blood-thinning medication.
iv. Important Safety Note: Warfarin and Vitamin K
If you take warfarin or another vitamin K antagonist, do not start vitamin K2 unless your anticoagulation clinic or prescribing clinician specifically advises it. Vitamin K can interfere with how these medicines work. This is one of the most important safety points in any article about Vitamin D3 and K2 for bone health.
v. Medical Treatments for Bone Loss
Depending on your risk, treatment may include:
- Vitamin D correction if deficient
- Calcium optimisation, preferably through food where possible
- Menopause hormone therapy, where appropriate
- Bisphosphonates
- Denosumab
- Selective oestrogen receptor modulators
- Parathyroid hormone-related treatments in higher-risk cases
- Fall prevention support
- Strength and balance training
The NICE BNF osteoporosis treatment summary notes that treatment often combines lifestyle changes and drug treatment to prevent fragility fractures. (British National Formulary)

Barriers and Challenges
i. “My Blood Tests Are Normal, So I Must Be Fine”
Routine blood tests do not always show bone loss. Calcium levels in the blood can look normal even when bone density is declining, because the body tightly regulates blood calcium. A DEXA scan is often needed to properly assess bone density.
ii. Confusing Supplement Marketing
Many products online promise stronger bones, hormone balance, or total menopause support. Some may be helpful, some may be unnecessary, and some may contain doses that are too high. This is why Vitamin D3 and K2 for bone health should be approached with curiosity and caution, not panic.
iii. Bone Health Is Often Discussed Too Late
Many women are not offered a bone-health conversation until after a fracture. But the best time to protect bone is before there is a crisis: during perimenopause, early menopause, pregnancy planning, postpartum recovery, or after starting medications that affect bone density.
iv. Diet and Access Challenges
Not everyone can easily meet calcium, vitamin D, protein, and vitamin K needs through diet. Vegan diets, lactose intolerance, food insecurity, digestive conditions, cultural dietary patterns, limited sunlight exposure, darker skin tone in low-sunlight climates, and covered clothing can all affect nutrient status.
v. Menopause Symptoms Can Distract From Bone Health
Hot flushes, poor sleep, anxiety, brain fog, weight changes, and heavy periods often take centre stage. Bone health can feel invisible because it does not always make a loud noise. But silent does not mean unimportant.
Solutions and Support
Food First Where Possible
A bone-supportive diet includes:
- Calcium-rich foods such as dairy, fortified plant milks, calcium-set tofu, sardines with bones, yoghurt, leafy greens, and fortified cereals
- Vitamin D sources such as oily fish, eggs, fortified foods, and supplements when needed
- Vitamin K sources such as leafy greens, fermented foods, and some animal foods
- Adequate protein to support muscle and bone
- Magnesium-rich foods such as nuts, seeds, beans, and whole grains
The NOGG osteoporosis guideline recommends a healthy, nutrient-rich, balanced diet and adequate calcium intake, preferably from dietary sources, with supplementation as needed. (NOGG)
Strength Training Is Bone Medicine
Bones respond to load. Weight-bearing and resistance exercises help maintain bone health. This may include:
- Brisk walking
- Stair climbing
- Resistance bands
- Weight training
- Pilates with appropriate loading
- Balance work
- Supervised strength programmes if you have osteoporosis or fracture risk
Supplements cannot replace the signal that muscles and gravity send to bone.
Menopause Care and Bone Protection
For some women, menopause hormone therapy may help protect bone density, especially when started around the menopause transition and when clinically appropriate. It is not suitable for everyone, and decisions should be personalised.
The British Menopause Society highlights osteoporosis prevention and treatment as part of menopause care and recognises the role of adequate calcium and vitamin D within a wider management plan. (British Menopause Society)
Smarter Supplement Use
A careful supplement plan may include:
- Checking whether you are actually deficient
- Choosing appropriate doses
- Avoiding very high-dose vitamin D unless prescribed
- Reviewing calcium intake before adding calcium tablets
- Considering K2 only if safe for your medication profile
- Rechecking blood levels when clinically advised
- Telling your clinician about all supplements
This is the balanced way to approach Vitamin D3 and K2 for bone health: informed, steady, and personalised.
Lifestyle Habits That Support Bone
Bone health is also supported by:
- Not smoking
- Limiting alcohol
- Eating enough protein
- Managing under-eating or restrictive dieting
- Treating heavy bleeding or anaemia
- Improving sleep
- Reducing fall risks at home
- Reviewing medications that affect bone density
- Getting medical support for gut conditions that affect absorption
Conclusion
Vitamin D3 and K2 for bone health matter because these nutrients support two essential parts of the bone-strength equation: absorbing calcium and helping activate calcium-handling proteins involved in bone mineralisation. But the real story is bigger than a supplement label.
Strong bones need enough nutrients, enough movement, enough hormonal support, and the right medical care when risk is higher. For women in perimenopause, menopause, post menopause, pregnancy, breastfeeding, or later life, bone health should not be an afterthought.
The goal is not to take every supplement on the shelf. The goal is to understand your risk, support your body wisely, and get help early enough to protect your future mobility, independence, and quality of life.
Takeaway
Your bone-health action box
- Know your risk: Ask about bone health if you have early menopause, fractures, steroid use, family history, low body weight, or malabsorption.
- Check before guessing: Vitamin D testing may be useful if you have symptoms or risk factors.
- Use supplements safely: Avoid high-dose vitamin D unless prescribed. Do not take K2 with warfarin unless your clinician advises it.
- Prioritise food and movement: Calcium, protein, vitamin D, vitamin K, strength training, and balance work all matter.
- Ask about a DEXA scan: Especially if you have menopause-related or medical risk factors.
- Think whole-body care: Hormones, gut health, sleep, muscle strength, and medications all affect bone.
Not sure where your symptoms fit? Take the Tools and Quizzes to understand your pattern.
Frequently Asked Questions
1. Is Vitamin D3 and K2 good for bone health?
Yes, Vitamin D3 and K2 for bone health can be helpful because vitamin D3 supports calcium absorption, while vitamin K2 helps activate proteins involved in calcium use in bone. But supplements should be matched to your needs and medical history.
2. Should I take Vitamin D3 and K2 every day?
Some people may benefit from daily vitamin D, especially during autumn and winter or if they are at higher risk of deficiency. K2 is less universally recommended, and you should avoid it if you take warfarin unless your clinician advises otherwise.
3. Can Vitamin D3 and K2 reverse osteoporosis?
No supplement should be presented as a cure for osteoporosis. Vitamin D3 and K2 for bone health may support bone metabolism, but osteoporosis often needs a broader plan that may include medication, menopause care, strength training, fall prevention, and monitoring.
4. What is the best time to take Vitamin D3 and K2?
Both are fat-soluble vitamins, so they are often taken with a meal that contains some fat. The exact timing is less important than consistency and safe dosing.
5. Do I need calcium with Vitamin D3 and K2?
Maybe. Vitamin D helps absorb calcium, but whether you need calcium supplements depends on your diet and risk level. Many people should aim to get calcium from food first, adding supplements only when intake is low or when clinically advised.
6. Who should be careful with Vitamin K2?
Anyone taking warfarin or another vitamin K antagonist should not start K2 without specialist advice. People with kidney disease, clotting disorders, complex medication regimens, pregnancy, or significant medical conditions should also check first.
7. Can low vitamin D cause bone pain?
Low vitamin D can contribute to bone pain, muscle weakness, and poor bone mineralisation in some people. But these symptoms are non-specific, so persistent pain or weakness should be medically evaluated.
Medical Disclaimer
This article is for educational purposes only and does not replace personalised medical advice, diagnosis, or treatment. If you are worried about your symptoms, if your symptoms are getting worse, or if something does not feel right in your body, please speak with your doctor, nurse practitioner, gynaecologist, endocrinologist, or another qualified healthcare professional. Seek urgent medical help for severe, sudden, or concerning symptoms.








